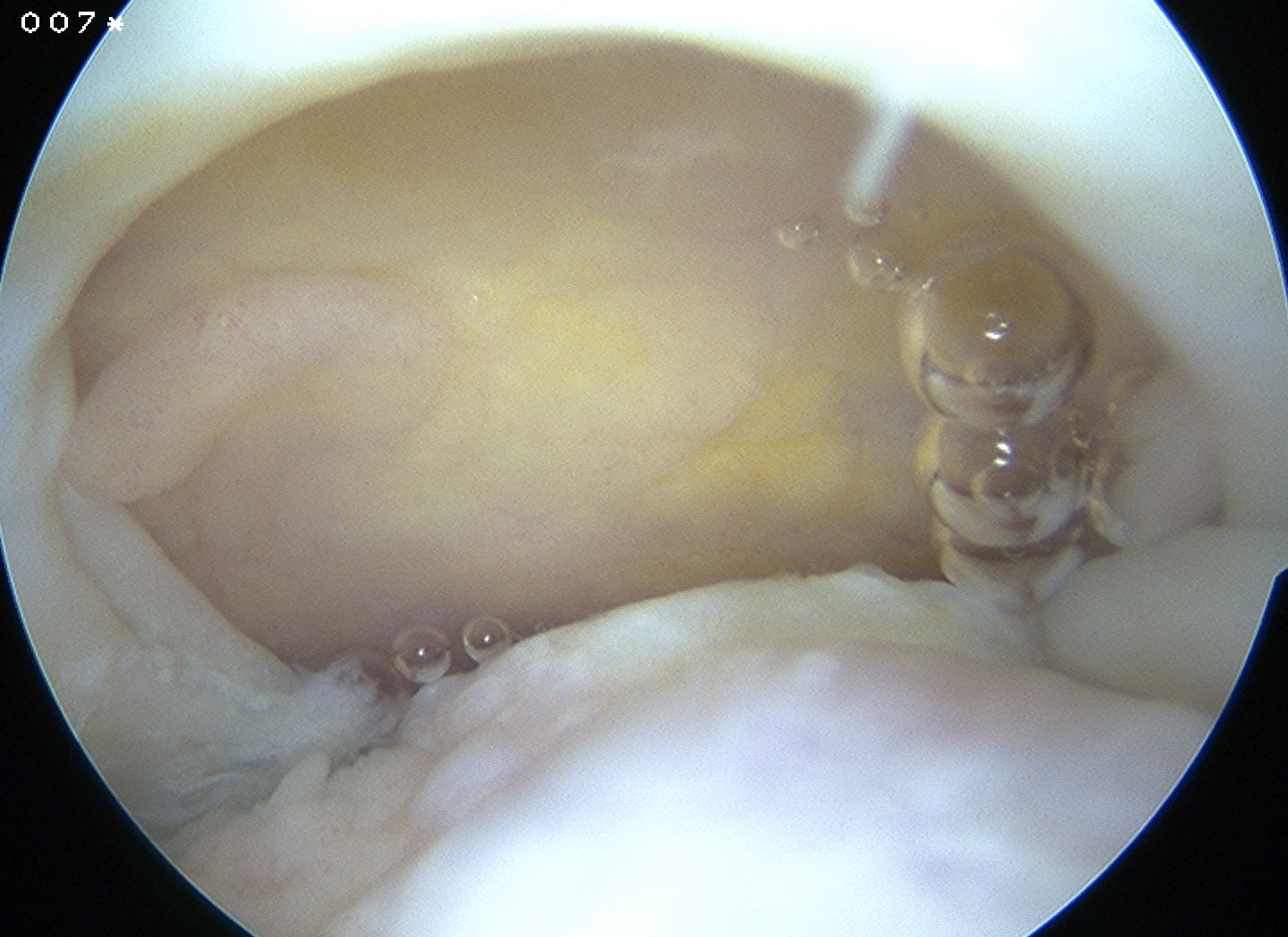
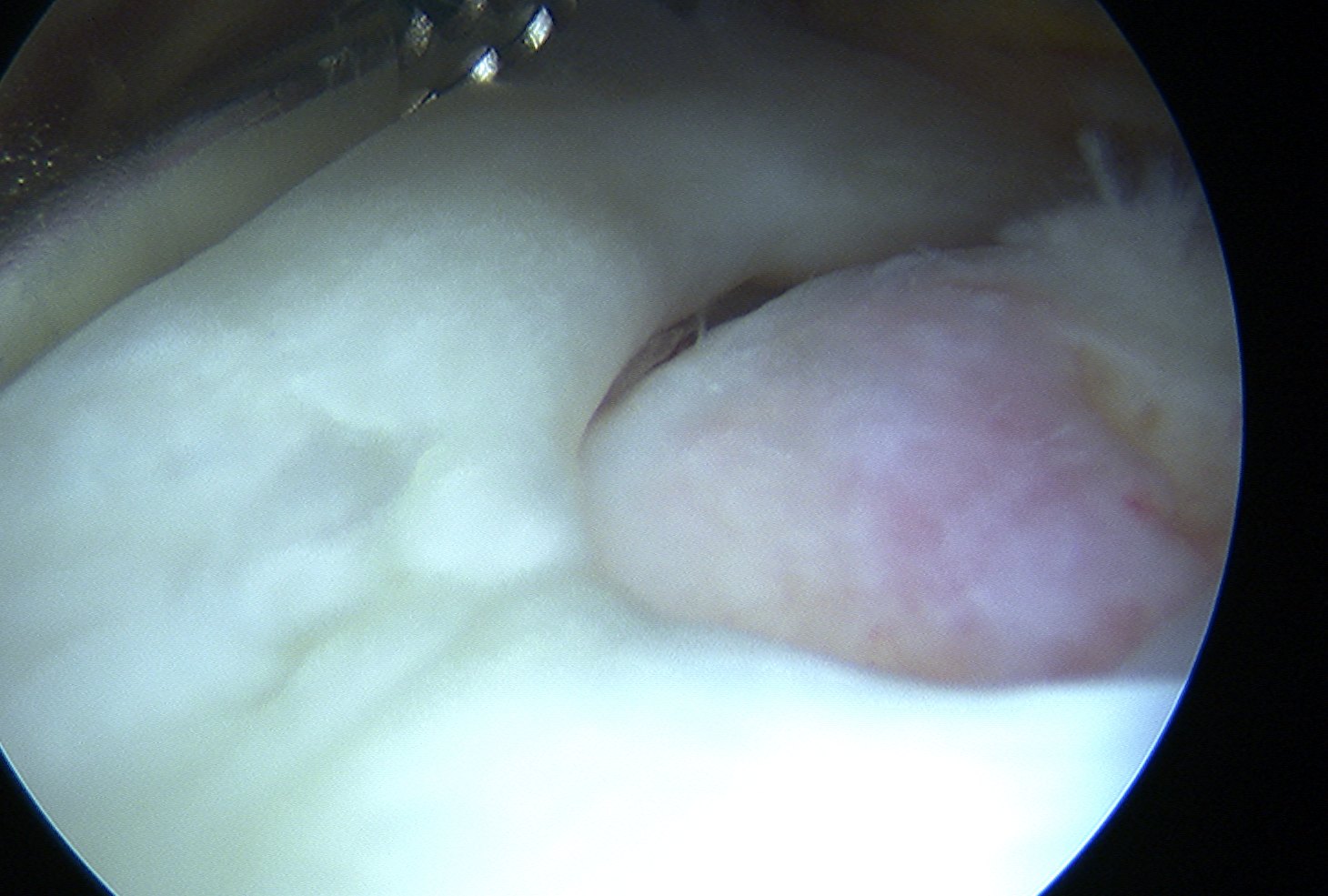
Arthoscopic Supraspinatous Repair
Advantages
Improved cosmesis
Improved cosmesis
TFCC tears
SL instability
Dorsal wrist ganglion
Scaphoid fracture with percutaneous pinning
Distal radius fracture
Tourniquet
Finger Traps Index & middle
Overhead traction device

2.7 mm scope / small joint instrumentation
- stabilise patient with beanbag or lateral rests
- apply skin traction to forearm
- place traction pole at foot of table opposite surgeon
- suspend arm with 10 lb weight
- abduction 60°
- forward flexion of 20°
- tilt top shoulder posteriorly 30° so that glenoid is parallel wwith bed
- mark bony landmark
- prep & free drape
Indications have narrowed
- due to success of shoulder arthroplasty
1. Chronic infections of GHJ
2. Stabilization in paralytic disorders
3. Post-traumatic brachial plexus palsy
4. Salvage of failed GHJ Arthroplasty
- may need bone graft procedures
5. Arthritic diseases unsuitable for arthroplasty / young patient
Post-traumatic (type III clavicle fractures)
Idiopathic
1. OA with osteophytes
- contribute to impingement

2. Osteolysis with resorption & gross osteoporosis
Intra-articular proximal ulna fracture
Articulates with trochlea
- may have a central bare area
Triceps insertion
- via broad aponeurosis which blends with anconeus and CEO
Undisplaced fracture
- need to ensure triceps mechanism is intact
Very few
- young labourer with severe disabling elbow pain
- trial in POP at 90o for 6 weeks
Poor function
- adjacent joints cannot compensate for loss of function
RA
- high failure rate especially flail elbow with poor bone stock

Templating
Approach
Fixation
Bearing Surface
Head Size
Offset
Disabling hip pain
Severe functional impairment
Failed non operative management
Painless deformity
Severe LBP
- most common indication
Ipsilateral knee pain
- less beneficial
Malposition
- especially abduction
Absent abductor mechanism
Flail
Active infection
Insufficient bone stock
LLD
Average age 6 years
20% distal humeral fracture
- second most common elbow fracture after supracondylar
Pull Off
- more common
- fracture begins posterolateral metaphysis
- LCL, ECRL & ECRB attached to fragment
Push off
- varus force to extended EJ