Definition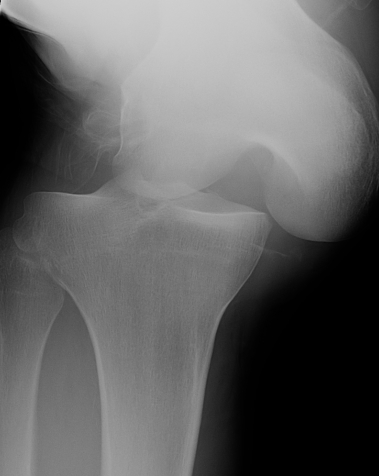
Multi-ligament knee injury (MLKI)
- 2 or more ligaments disrupted
Knee dislocation
- ACL + PCL + one of collaterals
Epidemiology
Male/Female: 4:1
Mechanism of injury
High energy (MVA)
Low energy (sport)
- low energy has 5% arterial injury
Ultra-low energy
- morbid obesity
- knee dislocation occurs with minimal trauma
Shenck Anatomic Classification 1992
KD-I: One cruciate + one collateral
KD-II: ACL and PCL torn
KD-IIIM: ACL / PCL + MCL
KD-IIIL: ACL / PCL + LCL / PLC
KD-IV: Both cruciates and both collaterals
KD-V: fracture dislocation
N nerve C arterial
Kennedy Classification
Based upon direction of the tibia
Anterior dislocation of tibia
- most common
- hyperextension + varus/valgus



Anterior knee dislocations
Posterior dislocation of tibia
- second most common
- flexed knee, posterior force
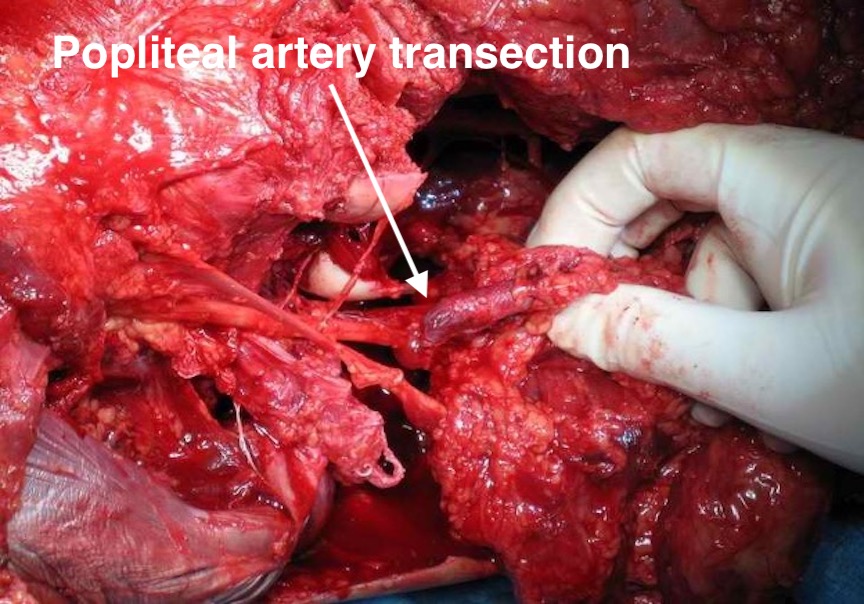
- high risk of popliteal artery transection


Posterior knee dislocations
Lateral dislocation of tibia
- KD-III L
- ACL / PCL / MCL
Lateral knee dislocation
Medial dislocation of tibia
- ACL / PCL / Posterolateral corner

Medial knee dislocation
Incidence
Rare
However incidence likely underreported
- many spontaneously reduce

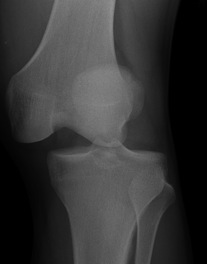
Obvious knee dislocation
Vascular Injury
Incidence
- systematic review of knee dislocation
- 171/862 (18%) had vascular injury
- 80% underwent repair
- 12% resulted in amputation
- most common in posterior dislocations (tibia) and with ACL / PCL / MCL
Anatomy
Popliteal artery tethered
- proximally in Hunters Canal under fibrous arch of adductor magnus
- distally under fibrous arch of soleus
- in middle by 5 geniculate arteries
Genicular vessels provide poor collateral flow
- amputation with vascular injury > 8 hours = 85%
More common in
- high energy injuries
- obese patients
Indications for vascular investigation
- angiography indicated if any of the three findings NOT PRESENT
- palpable dorsalis pedis, palpable posterior tibial artery, ABI > 0.9
Ankle brachial index (ABI)
Divide systolic pressure of the ankle by the systolic blood pressure of the arm
Options
CT angiogram
On table / vascular lab angiogram
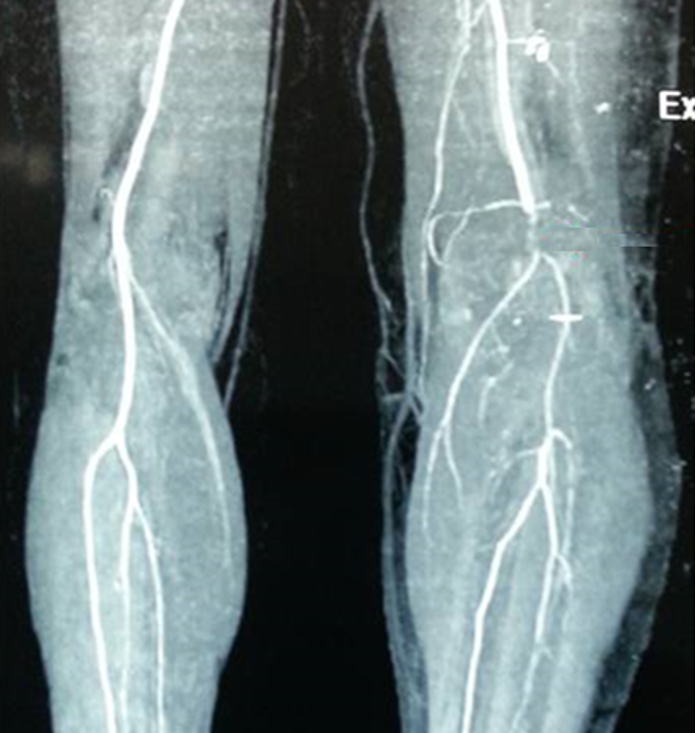
CT angiogram



Normal CT angiogram Popliteal artery stenosis following knee dislocation


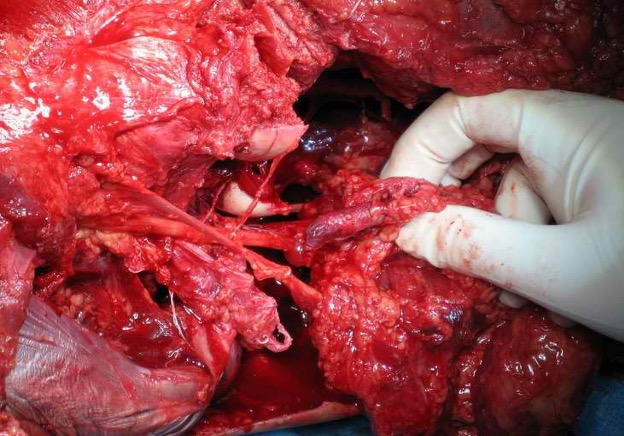
Popliteal artery transection following left knee dislocation
Advantages
- readily available, non invasive
- extremely accurate
- also used confirm the site and mechanism of injury
- multi-detector CT
- 100% sensitive and specific in detecting clinically significant arterial injury
Gakhal et al. Vascular and Interventional Radiology 2009
- CTA signs of lower extremity vascular trauma
Angiogram


Normal angiogram

Popliteal artery injury on angiogram
Disadvantages
- technically demanding
- potentially less accurate than CTA
- operator dependant
Technique
- open approach to proximal femoral artery
- place catheter in artery with 3 way tap
- 20mls Omnipaque / water soluble dye
- fluoroscopy over distal femur
- repeat for proximal tibia
- must show films to radiologist for interpretation of subtle signs
Rose et al. American J Roengenology 1987
- angiography 98% sensitive and specific for major arterial injury
- 16% technically compromised
Management of vascular injury
1. Bridging external fixation

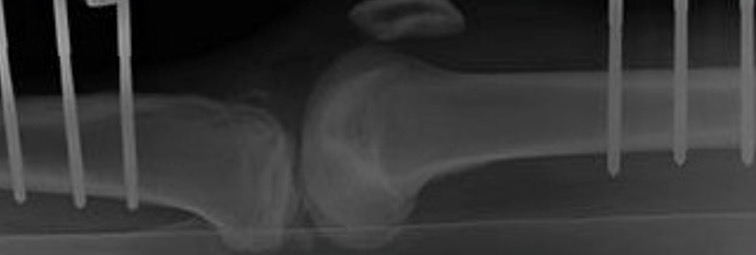

Bridging external fixator for knee dislocation
2. Vascular repair
Patient supine
- abduct hip, flex knee
- incision over sartorius proximally, running posterior border of knee
- detach medial head of gastrocnemius
- identify popliteal artery (medial) / popliteal vein / tibal nerve (lateral)
- reversed saphenous vein graft / synthetic graft
- fasciotomy if vascular injury - reperfusion raises risk of compartment syndrome
- apply external fixator - can flex but need to ensure that knee remains reduced

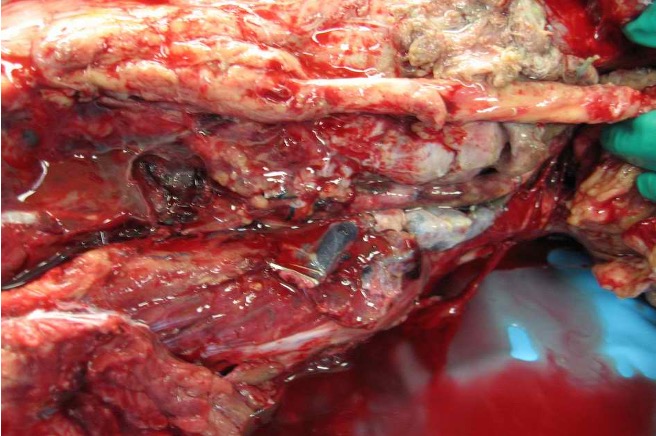
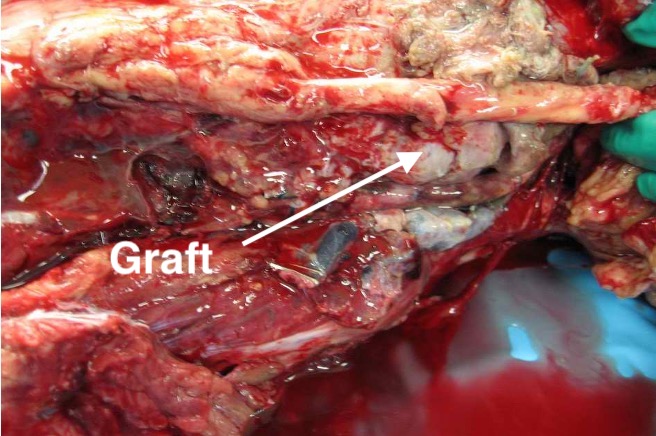
Medial approach and saphenous nerve graft for popliteal artery transection following knee dislocation
Nerve Injury
Incidence
- systematic review of knee dislocation
- incidence of nerve injury 25%
Patterns
1. Tibial nerve
- not tethered proximally
- not commonly injury
2. Common Peroneal Nerve
- tethered behind biceps and around neck of fibula
- most commonly injury
Prognosis
Woodmass et al Knee Surg Sports Traumatol Arthrosc 2015
- systematic review of 214 CPN palsies
- 40% of patients with complete nerve injury recovered foot dorsiflexion
- 87% of patients with partial nerve injury recovered foot dorsiflexion
Management options for CPN injury
1. Nerve obviously disrupted at surgery
- tag and return for sural nerve graft
2. Nerve intact
- EMG at 3 months
- if no evidence of re-inervation
- sural nerve gaft
3. Failure of sural nerve graft
- consider tendon transfers for foot drop
Samson et al EFORT Open Reviews
- management of CPN injury after knee dislocation
Examination
Extensive soft tissue injury with significant swelling
Open / compound wounds

Knee dislocation with obvious recurvatum and postero-lateral knee wound


Complete knee dislocation, compound, KDIV
Obvious ligamentous laxity


Excessive recurvatum Grade 3 Lateral laxity
Neurovascular status
- pulses, capillary refill, skin colour
- must have palpable dorsalis pedis, posterior tibial, as well as ABI > 0.9
- any concern, vascular investigation
Reduction of knee dislocation
Reduce in ER
- if stable can leave in brace
- if unstable, need external fixator
Dimple sign
Due to trapping of medial capsule & MCL
- after closed reduction of posterolateral dislocation
- get dimpling along the medial joint line
- MFC buttonholes through medial soft tisse
- non anatomic reduction achieved
- requires open reduction



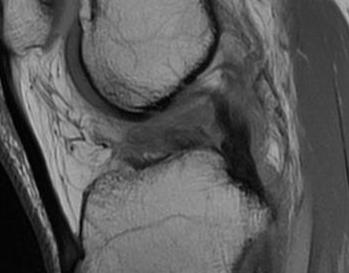
Medial dimpling Entrapped vastus medialis post knee dislocation on Coronal and Sagittal MRI

Open reduction of knee dislocation with medial approach and removal vastus medialis
External fixation
Indications
- open wounds
- unstable once relocated
- vascular injury
Associated Injuries
Fibula head avulsion / dislocation
Will typically have LCL and biceps femoris ligament attached


Fibular head avulsion

Fibula head avulsion and medial tibial plateau fracture
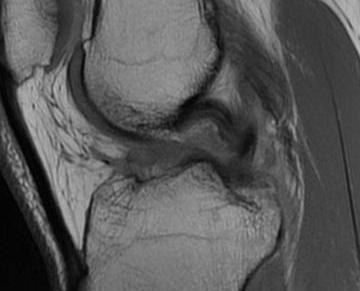
Patella fractures / extensor mechanism injuries
Sagittal MRI demonstrating patella tendon avulsion and ACL / PCL tear
PCL bony avulsions

Tibial plateau fractures


CT demonstrating medial tibial plateau in setting of knee dislocation and posterolateral corner injury
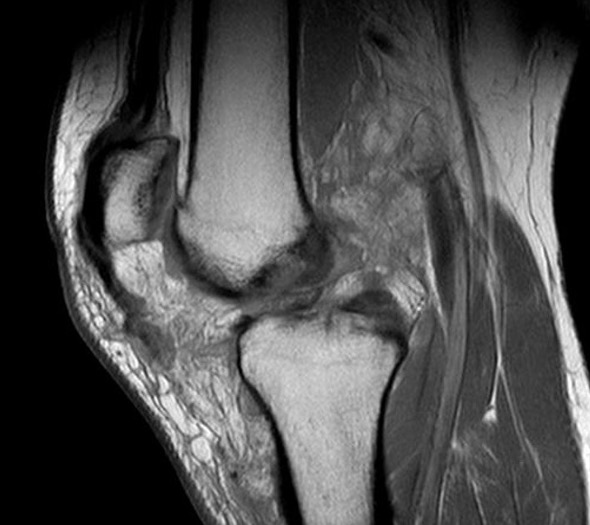
MRI
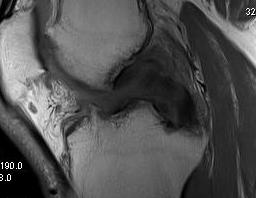
ACL / PCL rupture
Sagittal MRI demonstrating complete tear of ACL and PCL
Sagittal MRI demonstrating complete tear of ACL and mid substance tear of PCL
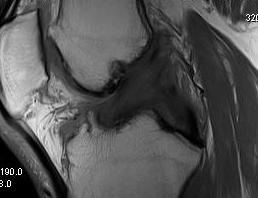
ACL / PLC / MCL


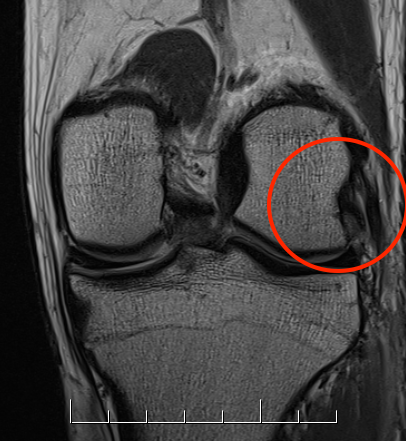
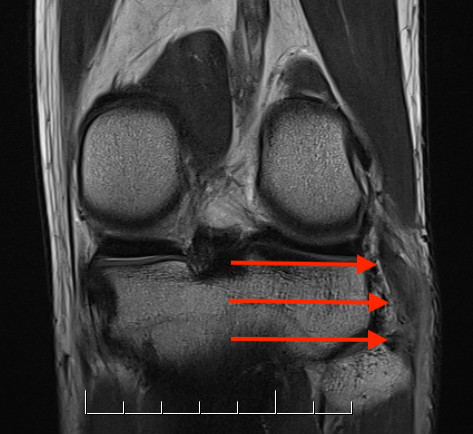
Coronal MRI of left knee demonstrating proximal MCL tear, with sagittal demonstrating complete disruption of ACL / PCL
Popliteus


Coronal MRI of left knee demonstrating femoral avulsion of popliteus
LCL
Harder to see on a single image. Need to scroll through coronal images

Coronal MRI with normal femoral insertion of LCL and popliteus

Coronal MRI of same patient demonstrating distal LCL avulsion from fibula