Forearm Fractures
Anatomy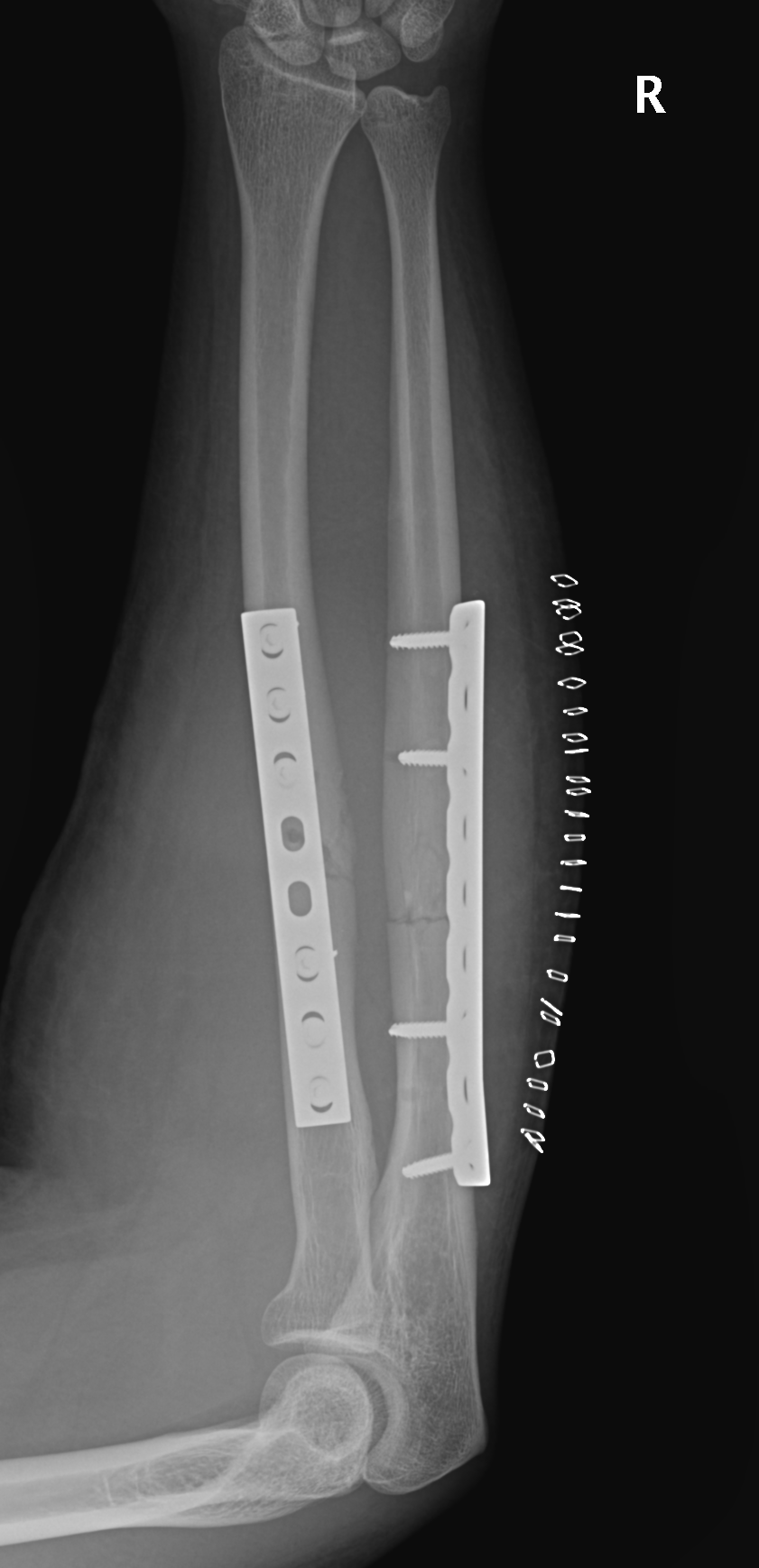
Radial bow radius
- important for rotation
Interosseous membrane
- Z pattern
- proximal radius to distal ulna
Mechanism
Direct blow
- ulna / night stick

Radial bow radius
- important for rotation
Interosseous membrane
- Z pattern
- proximal radius to distal ulna
Direct blow
- ulna / night stick
Usually occurs in young people
- often previous history of tendonitis ± steroid injections
Usually at level of inferior pole of patella
- less common at tibial tubercle
- mid-substance ruptures rare
Severe pain
Palpable defect
Extensor deficit / unable to SLR
Patella alta / high riding patella

Increased pressure within a closed fibro-osseous space
Seen in athletes, associated with repetitive exertion
Leg
1. Anterior compartment
- anterior tibial artery
- deep peroneal nerve
Most common in lateral meniscus 9:1
Peak incidence 20-40
Probably 2° to infiltration of joint fluid into extra-articular tissues
- almost always associated with horizontal cleavage tear
- creates a flap valve in lateral 1/3 of LM
Usually present with pain
- activity related
May notice lump
Natural History of ACL deficient knee is variable
- functional instability 15% - 90%
- progression to OA is variable
Depends on level of patient demands / activity
1. Late meniscal injury in ACL deficient knee
15-25%
2. Function
Daniels Am J Sports Med 1994
- 292 ACL defecients knees
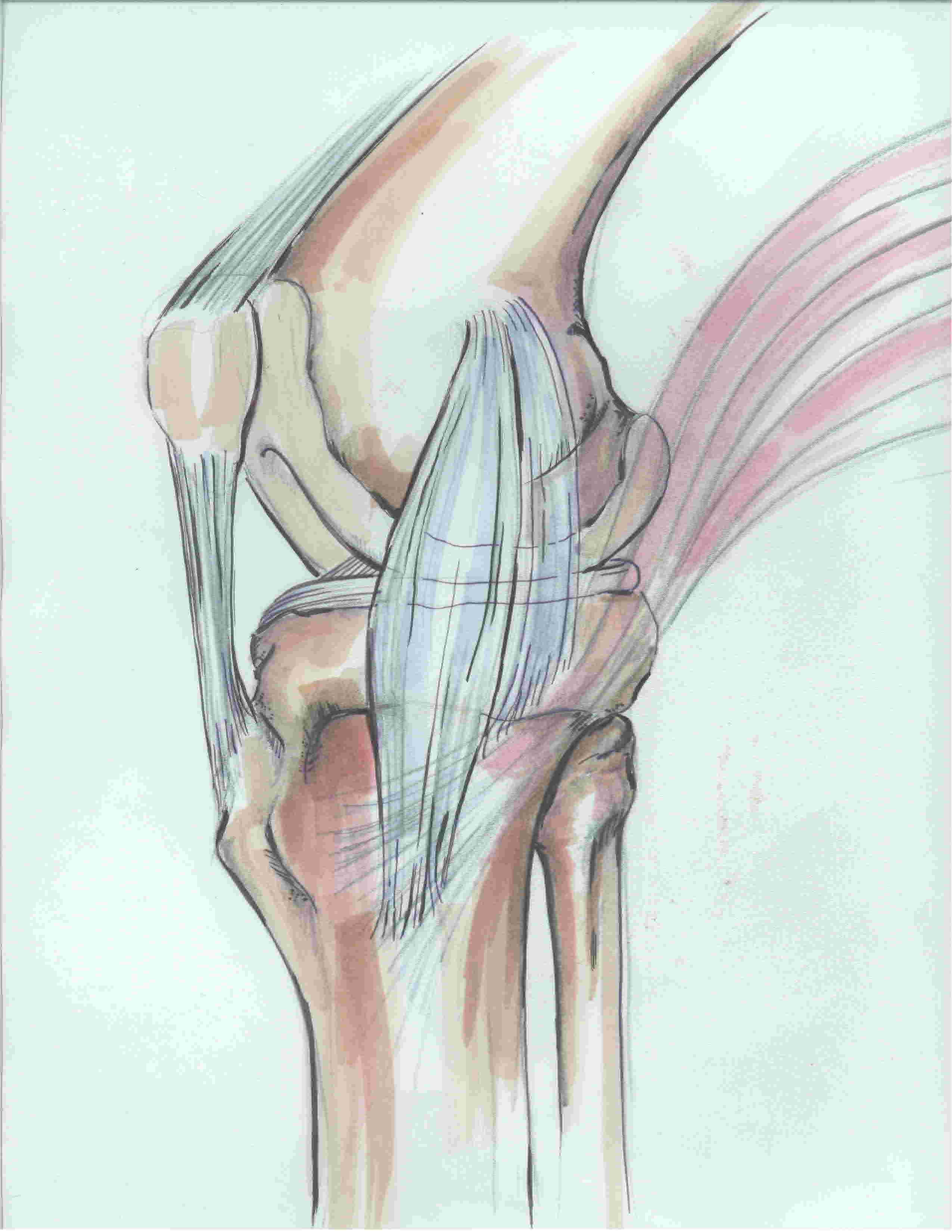
1. Seebacher's 3 layers of the medial knee
Layer 1
- sartorius and sartorius fascia
Layer 2
- superficial MCL
- posterior oblique ligament
- semimembranosus
Layer 3
- deep MCL (meniscofemoral and meniscotibial ligament)
- posteromedial capsule
2. MCL
Superficial MCL
Most common reason for litigation against orthopaedic surgeons in THR
Usually from lengthening
1. Nerve palsy
Sciatic nerve - tolerate average 4.4cm lengthening
Common peroneal nerve - tolerate average 2.7 cm lengthening
Lengthen by up to 15-20% of the resting nerve length
- but in reality is unknown and multifactorial

2-3% of cases
- doubles with infrequent operator
- second most common reason for revision after loosening
Australian Joint Registry
- dislocation accounts for 14.8% of revisions
Posterior dislocation
- hip flexed, adducted, IR

FOOSH
Age 6 as maximum ligamentous laxity
- < 4 - physeal separation
- > 8 - dislocation
Male > F
Supracondylar region in 6 year old is thin
- thinnest at olecranon fossa (2-3 mm)

Age 0 - 5
- Salter Harris I
Age 5 - 11
- Salter Harris II
III / IV rare
Great remodelling potential
- 80% growth of humerus from proximal physis
Shoulder ROM compensatory
Age
- even older adolescents do well