Fibula fractures
Weber Classification of fibula fractures
RA
OA
AVN
Infection
Charcot
Paralysis of deltoid
Torn rotator cuff
Insufficient glenoid bone stock
1. Significant functional impairment
2. PIPJ contracture
- originally thought to intervene early
- Macfarlane showed residual FFD always about 30o
- may need to release check rein ligaments / accessory collateral ligaments
3. MCPJ contracture >30o
4. Trigger fingers
- must do limited fasciectomy
Osseous canal between talus and calcaneum
- interosseous talo-calcaneal ligament
- cervical ligament
- joint capsule
- nerve endings / arterial anastomoses

Flat foot / overpronation
Inversion / sprain
Proximal tibia
- gastrocnemius local muscle flap
- gracilis free muscle flap if gastroc damaged
Middle tibia
- soleus local muscle flap
- gracilis free muscle flap
Distal tibia
- posterior tibial fasciocutaneous local flap
- gracilis free muscle flap

Usually young patients
- 15 - 40
15% compound
High velocity injury
- MBA
- MVA
- pedestrian v car
- fall from height
EMST principles
- need for transfusion not uncommon
1. Open antero-lateral approach
Large / Massive Cuff Tear
2. Deltopectoral approach
Large Subscapularis tear
3. Arthroscopic Assisted Mini-open
Indication
- Small / Moderate Cuff Tear < 3cm
- no retraction
Technique
- arthroscopic SAD

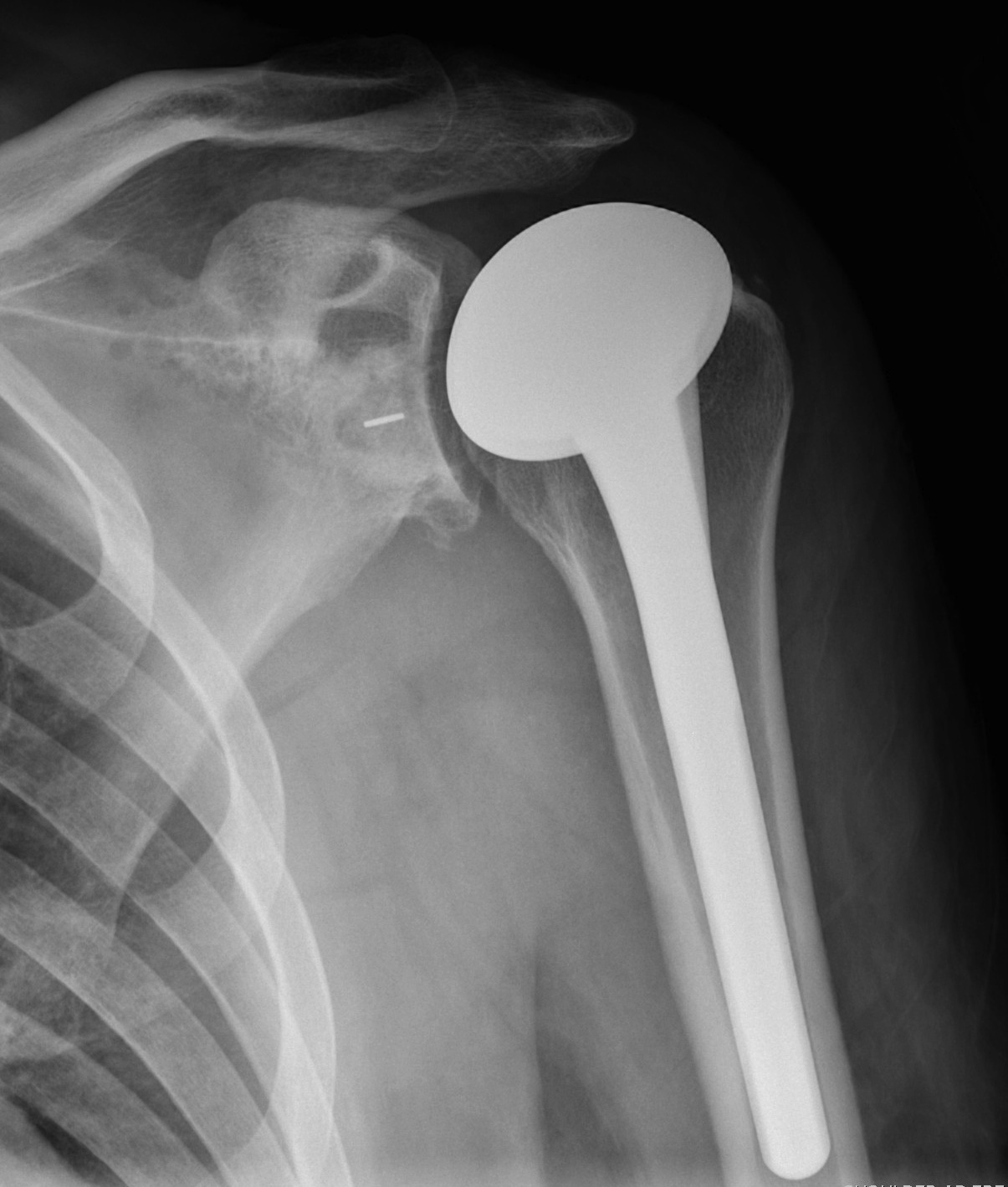
Rotator cuff
- often deficient
Bone stock
- often deficient
Glenoid
- often posterior version
1. TSR
Indications
- cuff intact

Male & Females > 60 years
- X-ray evidence of OA
Symptomatic
- 25% females
- 15% males
Base thumb
PIPJ / Bouchard's nodes
DIPJ / Heberden's nodes
Limb alignment
Risk that late posterolateral corner reconstruction will fail in the setting of the varus knee
- varus knee alignment and varus thrust in stance phase
- consider osteotomy first in this setting
Posterolateral Corner Reconstruction
Moulton et al. Am J Sports Med 2016
- systematic review of PCL reconstruction for chronic injuries
- 450 patients