
Goals of femoral cementing
Standard method (i.e. Exeter)
Optimize cement-bone interface
Cement mantle free of defects
Femoral component centered in cement mantle
Minimum 2 mm thickness
French paradox
Describes the stem inserted "line to line"
a thin mantle is generated in cancellous bone during pressurising
Design

Stryker Exeter Stem (taper-slip) Smith + Nephew Spectron (composite beam)
Taper-slip
- double or triple taper shape
- no collar
- highly polished (Ra < 1 micrometer)
- allows controlled subsidence in mantle (~1-2mm)
- continuously loading bone via hoop stresses
- no fixation between cement and stem (cement well fixed to bone)
Composite beam
- matte finish
- cement fixation between cement and stem (as well as cement and bone)
- no subsidence
- collared
Material
- Stainless steel
- generate less particulate debris than titanium
Cement Issues

Cement viscosity
- varying viscosity with different advantages
- low viscosity harder to handle early, but easier to inject (down a femur)
- high viscosity easier to handle
- no consensus in the literature regarding outcomes
Centrifugation / vacuum mixing
- reduces pore size
- stronger cement
- more resistant to fracturing
- reduces fumes
Pressurization
- pressurization increases penetration
- increases strength of cement-bone interface
Centralisers
- achieve more uniform cement mantle
- especially in zone 5 & 6
- prevent stress riser of tip of stem on bone
- allow controlled subsidence in a polished, taper-slip stem
Cement Mantle
- crack incidence greatest when mantle < 2 mm
- varus stem results in thin cement mantle in proximal medial & distal lateral zones
Antibiotics
- in relatively small doses effect on mechanical characteristics of PMMA negligible
- must be heat labile
- vancomycin / tobramycin / gentamicin
Cementing techniques
First-generation
- finger-packing doughy cement
Second-generation
- cement restrictor
- cleaning with pulsatile lavage
- cement inserted retrograde using cement gun
Third-generation
- vacuum centrifuge
- pressurization of cement mantle
Barrack's femoral component cementation quality grading system
| Grade | Definition |
|---|---|
| A | Complete filling of the medullary canal, without radiolucent lines between the cement and the bone (white-out) |
| B | Radiolucent line covering up to 50% of the cement-bone interface |
| C | Radiolucent line covering between 50% and 99% of the cement-bone interface or incomplete cement mantle |
| D | Complete radiolucent line (100%) at the cement-bone interface and/or absence of cement distally to the end of the stem |


Grade A Grade B Grade C Grade D
Techniques
Stryker Exeter surgical technique PDF
Zimmer CPT surgical technique PDF
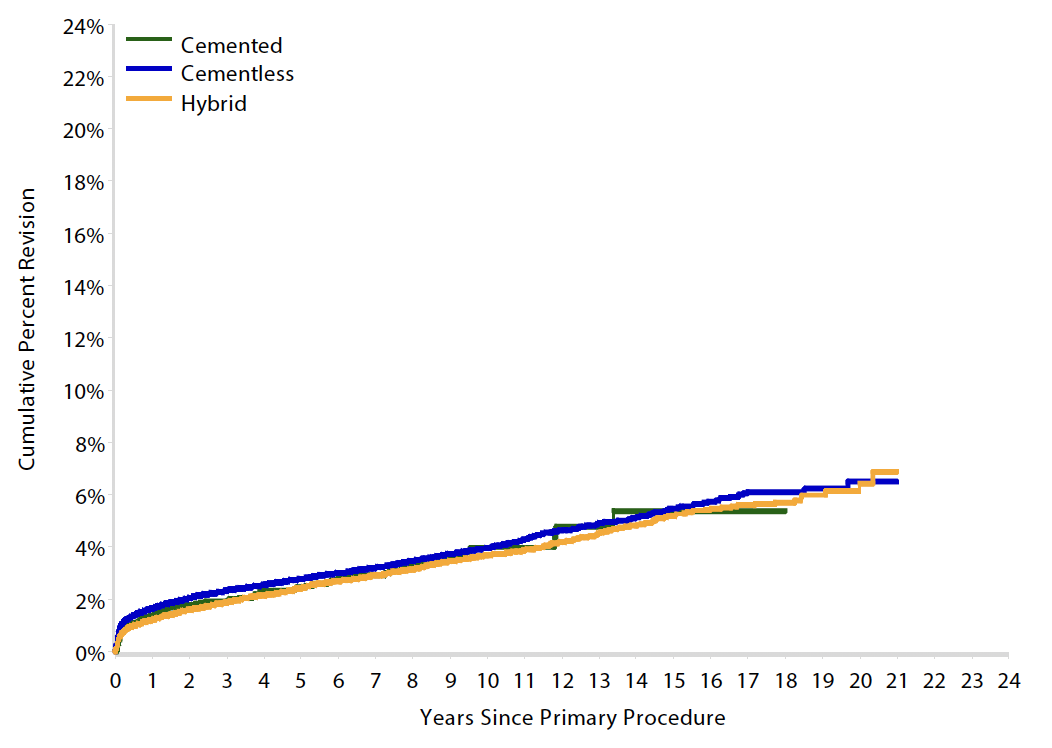
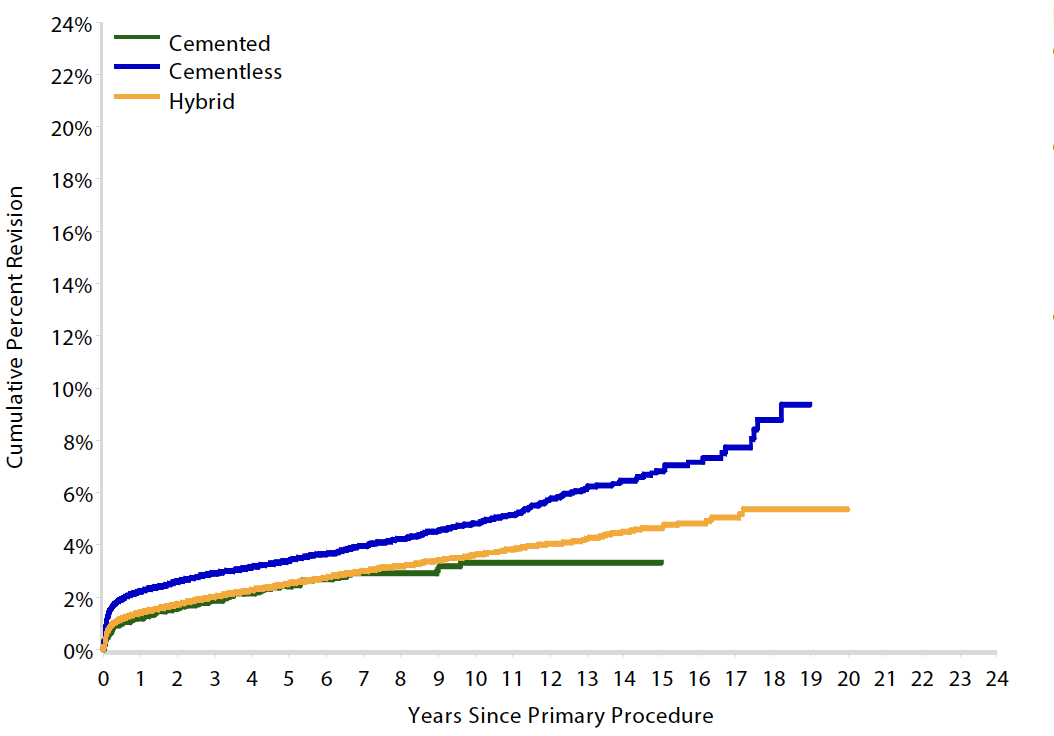
Results
Australian Joint Registry 2023 Revision rates by fixation (400,000 THA)
| Cemented | Uncemented | Hybrid | |
|---|---|---|---|
| 5 year | 2.6 | 3.0 | 2.6 |
| 10 year | 3.8 | 4.3 | 3.9 |
| 15 year | 5.1 | 5.9 | 5.3 |
| 20 year | 7.0 | 6.7 |
15 year revision rate by age
64 - 74 year > 75 years
| Cemented | Uncemented | Hybrid | |
|---|---|---|---|
| < 55 | 6.4 | 7.2 | |
| 55 - 64 | 6.2 | 5.5 | 6.1 |
| 65 - 74 | 5.4 | 5.5 | 5.2 |
| > 75 | 3.3 | 6.8 | 4.7 |
Complications
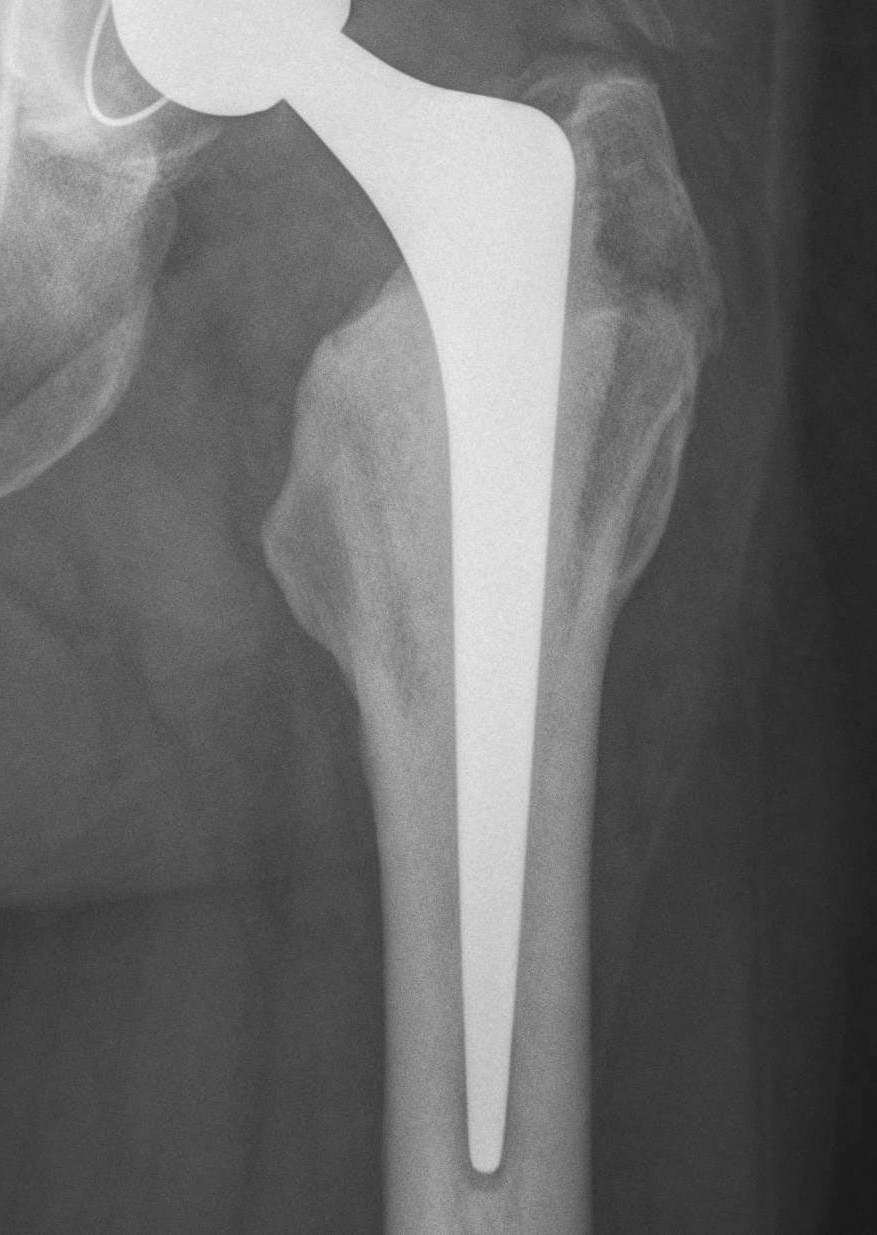
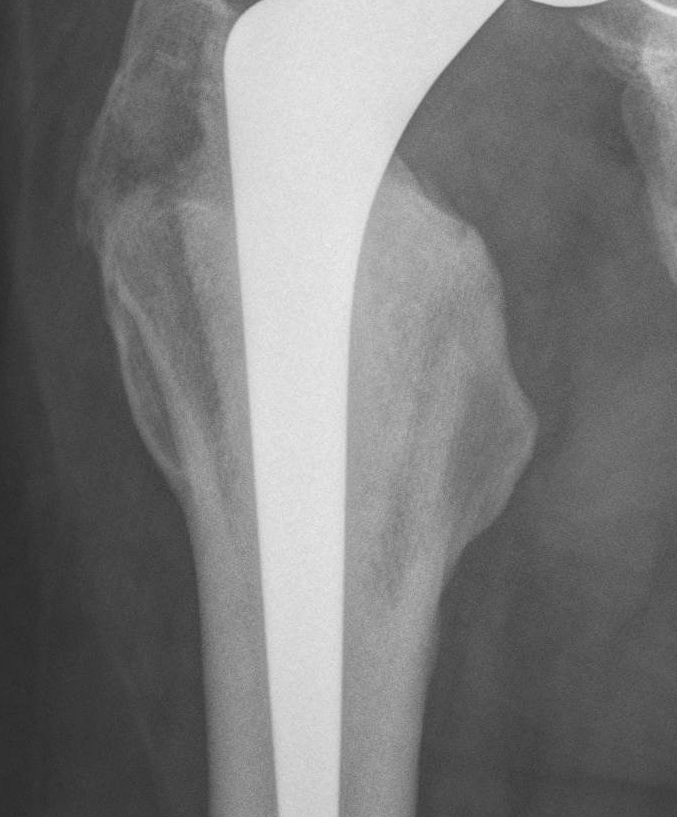
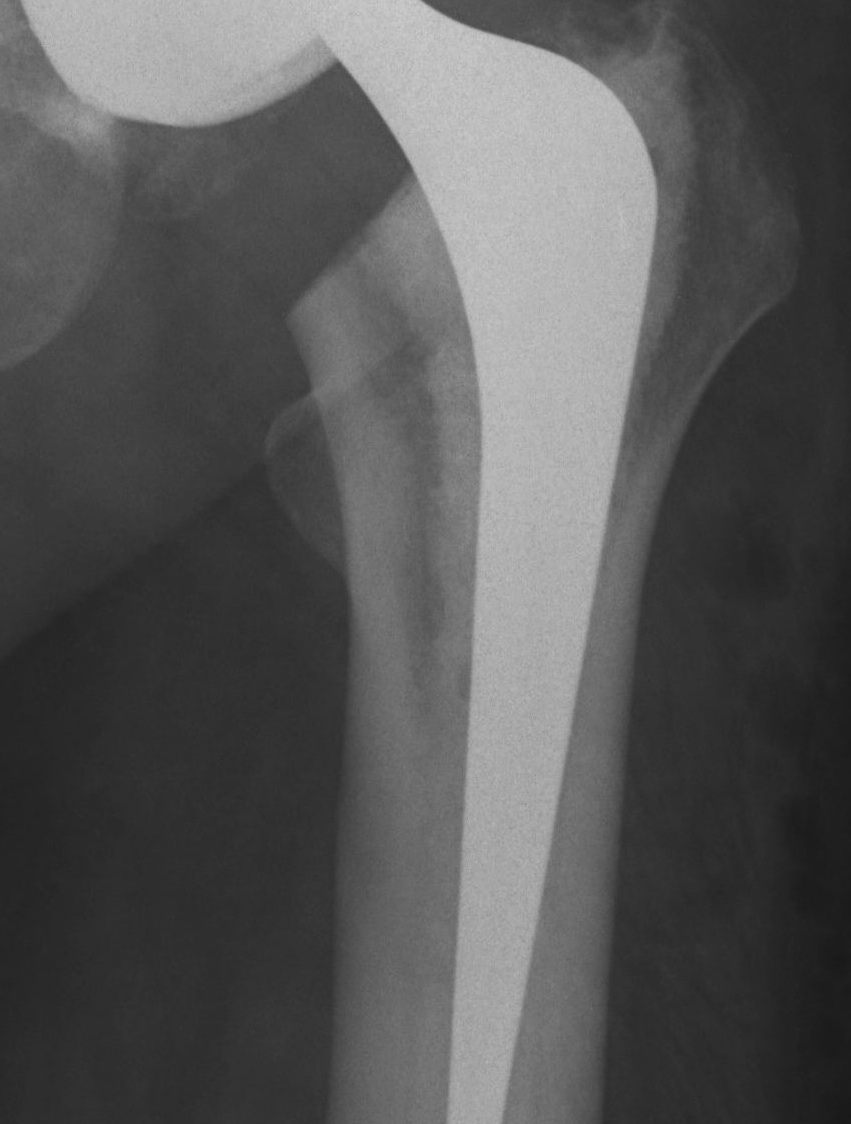
Loosening
Harris Categories of Cemented Femoral Stem Loosening
| Definitely Loose | Probably Loose | Possibly Loose |
|---|---|---|
|
Change in stem position
Cement mantle fracture
Radiolucent line > 1 mm |
Lucencies at cement implant interface
Endosteal scalloping |
Radiolucent lines at cement/bone interface |


Definitely Probably Possibly