Concept
Treat the wound, not the gun velocity
Management based on gun velocity old fashioned because
1. Only 1/3 guns are known
2. High velocity guns can produce low energy transfer wounds
Wound Ballistics
Kinetic Energy = 1/2mv2
- important factor is tissue interaction
- energy transfer
Two mechanisms of tissue injury
1. Permanent cavity
- tissue actually hit by the bullet
- increases with distance travelled through tissue
2. Temporary cavity
- tissue stretched by the bullet passage
- as vacuum created, microbes can be sucked in at exit or entry
- increased with distance travelled through tissue
Microbes
Bullets are not sterile
- suck microbes in as well
- clothing fabric gets pulled in too
- wadding also gets into wound
Pathology
Amount of tissue damage depends on
1. Bullet type
- partially jacketed fall apart
- Dum Dum - soft nosed bullets deform and start to spin earlier
2. Target tissue
- inelastic brain worse than elastic muscle
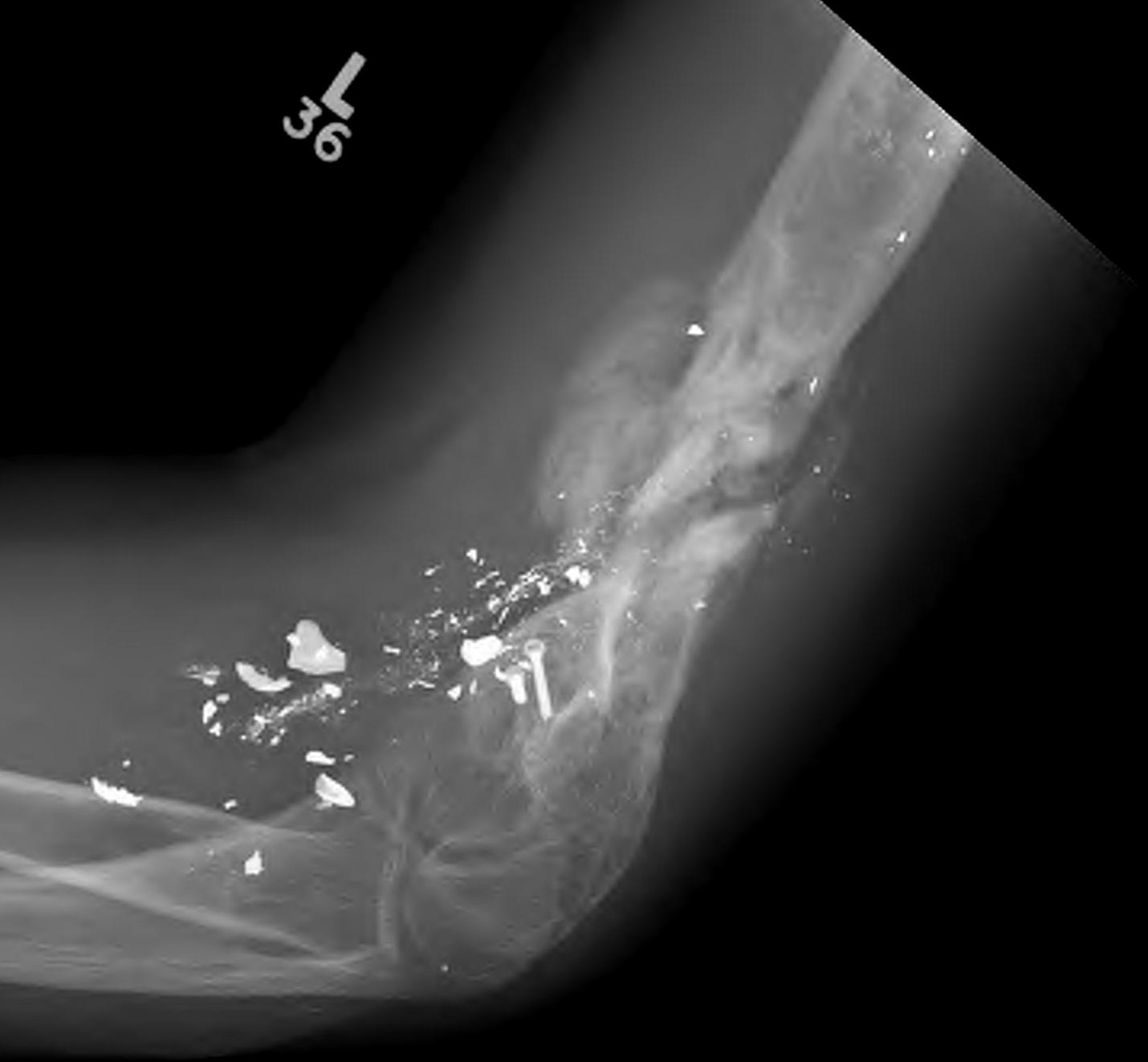
- bone fragments can produce their own injury
3. Tissue width
- bullets really cause damage after they spin 180°
- occurs when hit tissue
- has to be > 12cm tissue thickness for this to start
- hence calf may have low energy transfer wound
- thigh / abdomen have high energy transfer
- energy transfer can increase as travel along wound
4. High velocity bullets
- have more kinetic energy to transfer
- much worse if start to spin / > 12 cm tissue
- better outcome if already exited prior to spin or fragmentation
Management
Initial
ATLS
- secondary survey
- entry wound / exit wound
- NV injury
- history gun type & range
- cover wound
- ADT & antibiotics
- splint
Abdomen
- all GSW that pass through the abdomen become infected without 2/52 antibiotic treatment
Lumbar spine
- all bullets retained in the lumbar spine should be removed acutely
- the cauda equina involves multiple levels & LMN have a better chance of recovery
- better if < 48/24 or > 2/52 to avoid oedema
Operative Management

First OT
- scrub
- large incisions to explore wound
- excise all devitalised tissue
- washout +++
- skeletal stabilisation
- always leave wound open
Remove bullet if
- easy to do so
- danger of later migration causing injury
- likely to cause later pain (i.e. hand / foot)
Second OT
- 48 hours
- DPC if wound clean
- SSG / muscle flaps as needed
Non-Operative Management
In USA good success with non-op management of low energy transfer wounds