Definition
Bunion
- medial prominence of head of 1st MT
Hallux Valgus
- medial deviation 1st MT
- lateral deviation of great toe
Anatomy
Metatarsal head
- has 2 grooves separating ridge (cristae)
Sesamoid
- in each tendon of FHB
- sesamoids attach to P1
- no attachment to MT head
- sesamoid ligaments attach to sesamoids and plantar plate
- FHL passes plantar to the plate & between the sesamoids
Plantar plate
- formed by
- FHB / Abd. Hall / Add. Hall / Plantar aponeurosis / capsule
Sesamoids and plantar plate stabilised
- abductor hallucis (medial)
- adductor hallucis & trans metatarsal ligament (lateral)
- insert into sesamoids & Base P1
- no muscles insert into head MT
Collateral ligaments
- from head of MT to base of P1
- insert into sesamoids
Biomechanics
Great Toe provides stability to the medial aspect of the foot
Windlass mechanism of plantar aponeurosis
- plantar aponeurosis arises from tubercle of calcaneum
- medial slip inserts into base of proximal phalanx via sesamoids
- as body passes over foot, P1 forced into DF & slides over MT head
- plantar aponeurosis winds around MT head & plantarflexes the 1st MT
- creates arch
In hallux valgus, windlass is less effective
- results in transfer of weight to lateral aspect of foot
- especially second MT head
Blood Supply
3 main
- 1st dorsal and plantar metatarsal artery
- superficial branch of medial plantar artery
Medial
Medial plantar artery
- remains plantar to the MT until the level of the neck when it runs obliquely dorsally
- divides into the medial cervical branch, and the medial sesamoid branch
Lateral
First plantar MT artery
- is formed by the deep plantar arch and a perforating branch from the DPA
- runs distally in the 1st MT space
- nutrient artery to neck (variable)
- cervico-sesamoid branch (constant)
Lateral Cervical branch
- enters plantar surface at base of neck
- supply major part of head
- care in not stripping under the neck to preserve the cervical branch
Dorsolateral
- small branch from DPA
- penetrates the dorso-lateral capsule near margin of articular cartilage
- not big enough to provide sole supply
- can be sacrificed if needed
Characteristics
Great toe
- lateral deviation of the great toe (HVA > 15o)
- medial deviation of the first metatarsal (IMA > 9o)
- +/- subluxation of the first MTPJ
- hallux pronation
- prominent mediation eminence
- sesamoid rotation / uncovering
Lesser toes
- overriding of the second toe
- metatarsalgia
- lesser toe hammer & claw
Epidemiology
Two ages of presentation
1. Adolescent form
- usually bilateral
2. Adult form ~ 50's
- strongly familial
- positive FHx in 2/3
- F > M
- F:M = 9:1 in those needing operations
Aetiology
Likely multifactorial
1. Shoe Wearing
Evidence
- more women are affected
- women's shoes are tight-toed
- unshod 2% vs 33% shod
- unshod toes separate on weight bearing
- in shoes, toes crowded & hallux abducted
2. Hereditary
- usually strong FHx
- tend to present earlier
- AD with incomplete penetrance
- made worse by female's shoe wear
3. Generalised Ligamentous Laxity
- splaying of forefoot
- excessive mobility of 1st TMT
- laxity of medial capsule of MTPJ
4. Anatomical factors
Metatarsus Primus Varus
- associated with HV
- especially adolescent variety

1st MT
- long / short
- hyper pronated
2nd Toe amputation
- loss of lateral support for great toe
MTPJ
- rounded joint
TMTJ
- hypermobile
- medially slanted
Flatfoot
Short achilles tendon
5. Pathological Conditions
Rheumatoid arthritis
- leads to loss of capsular support
- RA best treated with fusion
Neurological conditions
- CP best treated with fusion
Pathology
A. Congruent MTP joint
Cause
- increased DMAA
- Hallux valgus interphalangeus
Present
- enlarged medial eminence (bunion)
- pressure against shoe
- painful bursa or cutaneous nerve
Management
- MTP joint usually stable & won't sublux
- can’t do distal soft tissue release
- will sublux a congruent joint
B. Incongruent MTPJ
 , ex
, ex
Subluxed MTPJ
- usually progressive
Origin
- starts with lateral pressure on great toe
- tight high heels
- P1 moves laterally
Progression
- PI moves laterally & puts pressure on MT head
- moves it medially, thus increasing intermetatarsal angle
- attenuation of medial joint capsule
- sesamoid sling held in place by ADDH & transverse metatarsal ligament
- MT head moves further medially / varus deformity
- slides off sesamoids
Final deformity
- appearance of lateral migration of sesamoids
- however sesamoids maintain constant distance from second MT
- lateral sesamoid lies beside MT head in intermetatarsal space
- ADDH pronates the great toe
- medial extensor hood / capsule stretched
- EHL & FHL comes to lie lateral to MTPJ
- finally, lateral capsular structures become contracted & the deformity becomes fixed
C. Medial Eminence
- MT head changes occur
- groove or medial sagittal sulcus develops at medial border of articular cartilage
D. Bunion
- callosity of skin + bursa
E. Lesser Toes
- MTP less stable & weight transferred to MT 2 & 3 -> callosities
- great toe may drift beneath 2nd toe
- alternatively, 2nd toe may subluxate laterally
- lateral toes become crowded
- often develop claw or hammer deformity
- increased weight bearing through middle MT heads may lead to metatarsalgia
- worse with clawing of lesser toes
History
Pain
- over medial eminence (75%)
- metatarsalgia under lesser toes
- degeneration of sesamoid joint
- dorsal aspect osteophytes / rigidus
Shoe problems
- wide foot
- difficulty fitting shoes
Secondary deformity of lesser toes
- especially hammer deformity of the second toe
- rubbing of the PIPJ on shoe
Cosmetic appearance
Examination

Standing
- bunion
- HV
- clawing / hammer toes
Assess ROM ankle and STJ
- tight T Achilles
Look at wear patterns on foot
- callosities under 2/3 MT head
MTPJ
- tender bunion
- painful MTJP
- correctable / ROM correctable
- pain over sesamoids
TMTJ
- hypermobility
- > 9mm abnormal
Lesser toes
- deformity / correctable
Neurovascular examination
Weight Bearing AP X-ray
1. Hallux Valgus Angle / MTPA
- metatarso-phalangeal angle
- normal < 15o

2. Intermetatarsal angle/ IMA
- normal < 9o
3. Congruence
- place dots
- medial & lateral edges of the articular surfaces of the MT head & P1 base
- assess to see if line up / joint congruent
4. Interphalangeal angle
- normal is <10°
- identify hallux interphalangeus
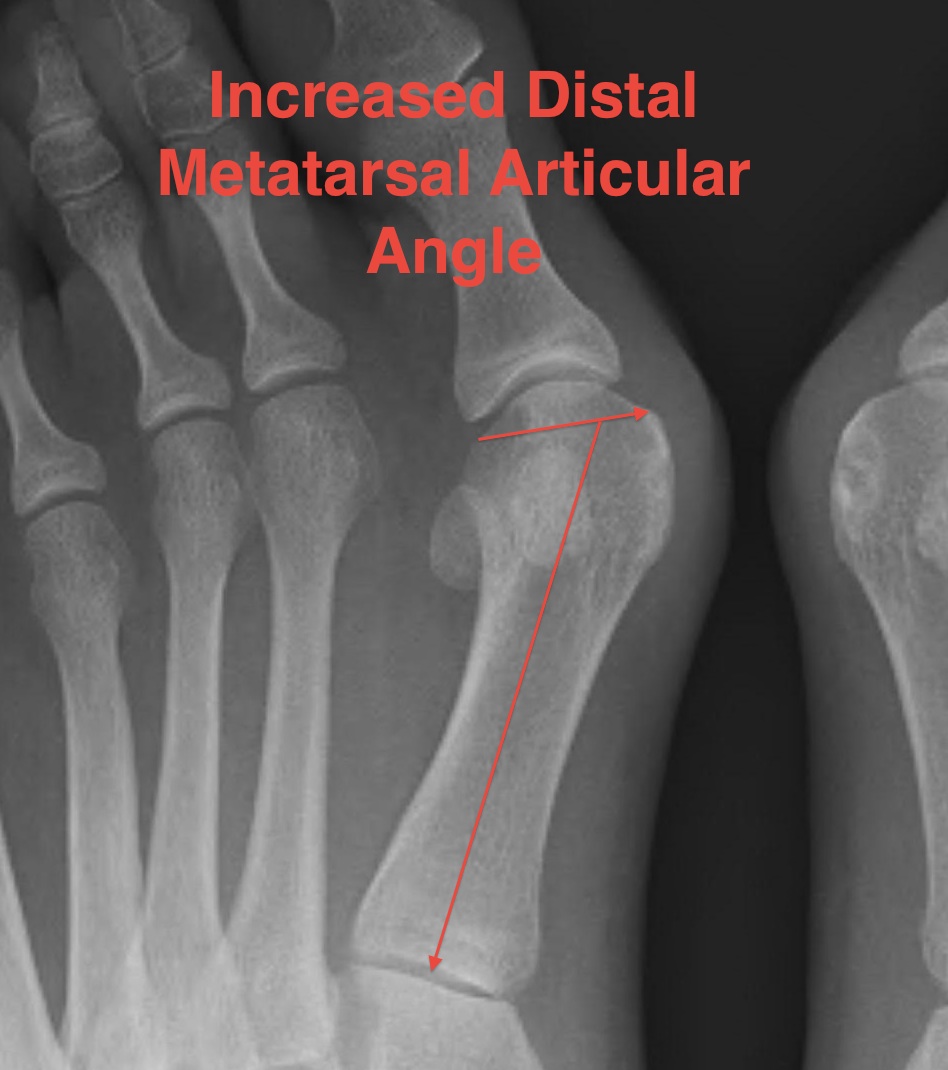
5. DMAA
- distal metatarsal articular angle
- normal < 6o
5. Sesamoid subluxation
- amount of lateral sesamoid uncovered by MT
- medial sesamoid should not cross midline axis of MT

6. MTPJ OA
7. Size of the medial eminence
- amount of MT head medial to the line along the medial border of the MT
8. TMT Angle
- medial sloping

Mann Classification
1. Congruent
2. Incongruent
A. Mild
MTPA < 30°
IMA < 15°
Lateral sesamoid < 50% uncovered

B. Moderate
MTPA 30 - 40°
IMTA 15 - 20o
Lateral sesamoid 50 - 75% uncovered
C. Severe
MTPA > 40°
IMTA > 20°
Lateral sesamoid > 75% uncovered

3. Degenerative