Definition
Abnormal development of acetabulum with decreased femoral head coverage
Aetiology
DDH
Perthes
SUFE
NMD e.g. cerebral palsy
Skeletal Dysplasia (MED etc)
Plus
- trauma
- infection
Epidemiology
Females > Males
- keeping with DDH
- males usually with other diagnosis
- considerable number are asymptomatic diagnosis on X-ray
Problem of late teens / early twenties
NHx
3 important factors
1. Degree of lateral subluxation
- CE < 20° = 80% OA
- unknown if covering head decreases OA
- 20 - 50% so called primary OA due to dysplasia
2. Young age
- acetabulum can remodel to age 5
- dysplasia improves only with concentric reduction
- most rapidly in first 6 months
3. Symptomatic
- natural history of asymptomatic subluxation is unknown
- likely to be much more benign
- it is known that early symptomatic acetabular dysplasia has a much poorer prognosis
- i.e. the twenty year old with a symptomatic hip will likely have severe arthritis in ten years
- untreated DDH said to lead to OA by age 50 in 50%
Weinstein JBJS July 2000
1. Subluxation
- all get severe OA & clinical disability
- age of symptoms depends on severity
2. Dysplasia
- NHx difficult to predict
- strong association between women & degenerative joint disease
3. Dislocated hips (untreated)
- may have no disability
- if have well developed false acetabulum may develop severe DJD
Clinical
3 peaks of patient presentation
- depends on degree of subluxation
1. Severe subluxation - patient in teens
2. Moderate subluxation - patient in 20 & 30's
3. Minimal subluxation - postmenopausal patients
Acetabular Rim Syndrome Ganz JBJS Br 1991
- patients with acetabular dysplasia found to have 20% incidence of labral tear
- complain of sharp knife like pain in groin and giving way or locking
- elicited by flexion and IR
- brings proximal & anterior femoral neck into contact with rim of acetabulum
- this is where labrum is likely to be damaged -> superolateral quadrant
X-ray Measurements
1. Shenton's Line
- Cooperman found it to be best prognostic sign
2. Acetabular Index
- paediatric
- triradiate cartilage to lateral edge of acetabulum
- birth 30°
- at 2 years - 20°
- N = < 30°
- DDH > 35°
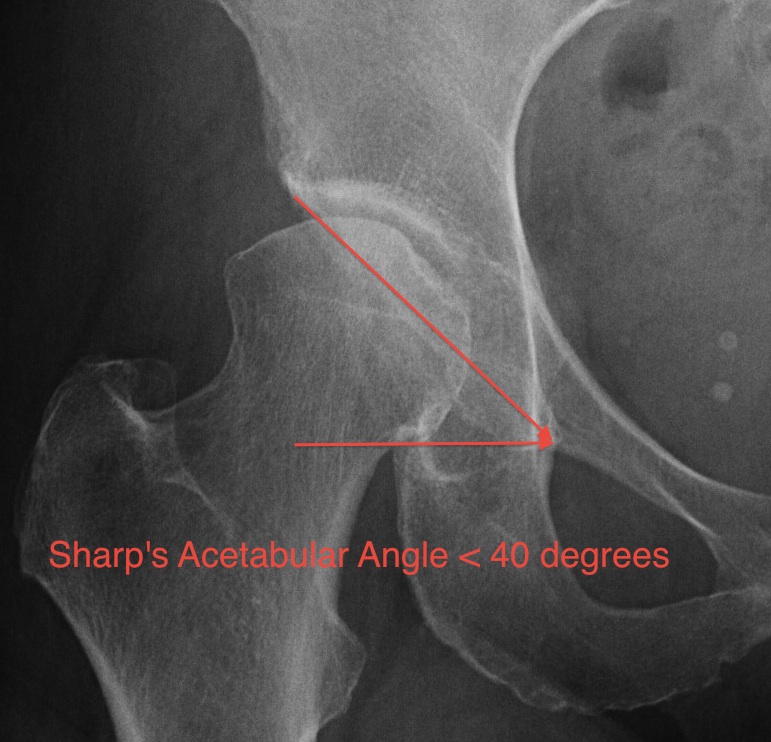
3. Sharp's Acetabular Angle 1961
- adult
- inferior tip tear drop to lateral edge acetabulum
- > 42° Abnormal
4. Centre Edge Angle of Wiberg 1939
- Perkin's line and line to centre femoral head
- < 20° abnormal / dysplasia
- > 40° Protrusio
- demonstrated increased increased of OA smaller the CE angle

5. Sourcil angle
- line of angle of sourcil (sclerotic weight bearing area of femoral head)
- horizontal line
- normal < 10°
- dysplasia > 10°

6. Weinstein Extrusion Index
- Head Covered / Total Width
- < 75% head covered abnormal
7. Lateral Subluxation
Teardrop to femoral head
Ganz Group I 13+/- 4mm
Group II 6+/- 2mm
8. Peak to Edge Distance
Ganz group I 3+/- 5mm
group II 16+/- 4mm
CT Reconstruction
Probably best anatomical view of hip prior to deciding on osteotomy
Management
Aim is to decrease cartilage stress below stress threshold
- by increasing joint surface area & decrease joint reaction force
- decreasing later OA & providing a painless functional joint
Controversy regarding treatment painless hip with CE < 20o
Options
1. Femoral osteotomy
- varising ostetomy
2. Acetabular osteotomy
- Reconstructive - Salter / Ganz
- Salvage - Chiari / Shelf
3. Both
4. Hip Arthroscopy
- debridement labral tear