Aetiology
Low Lesion (Below Elbow)
Injury usually at wrist
- laceration at wrist
- fenetrating forearm wound

High lesion / Above elbow
Injury usually at elbow
- elbow fracture / dislocation
- compression (GA)
- tardy ulna palsy
Low Lesion
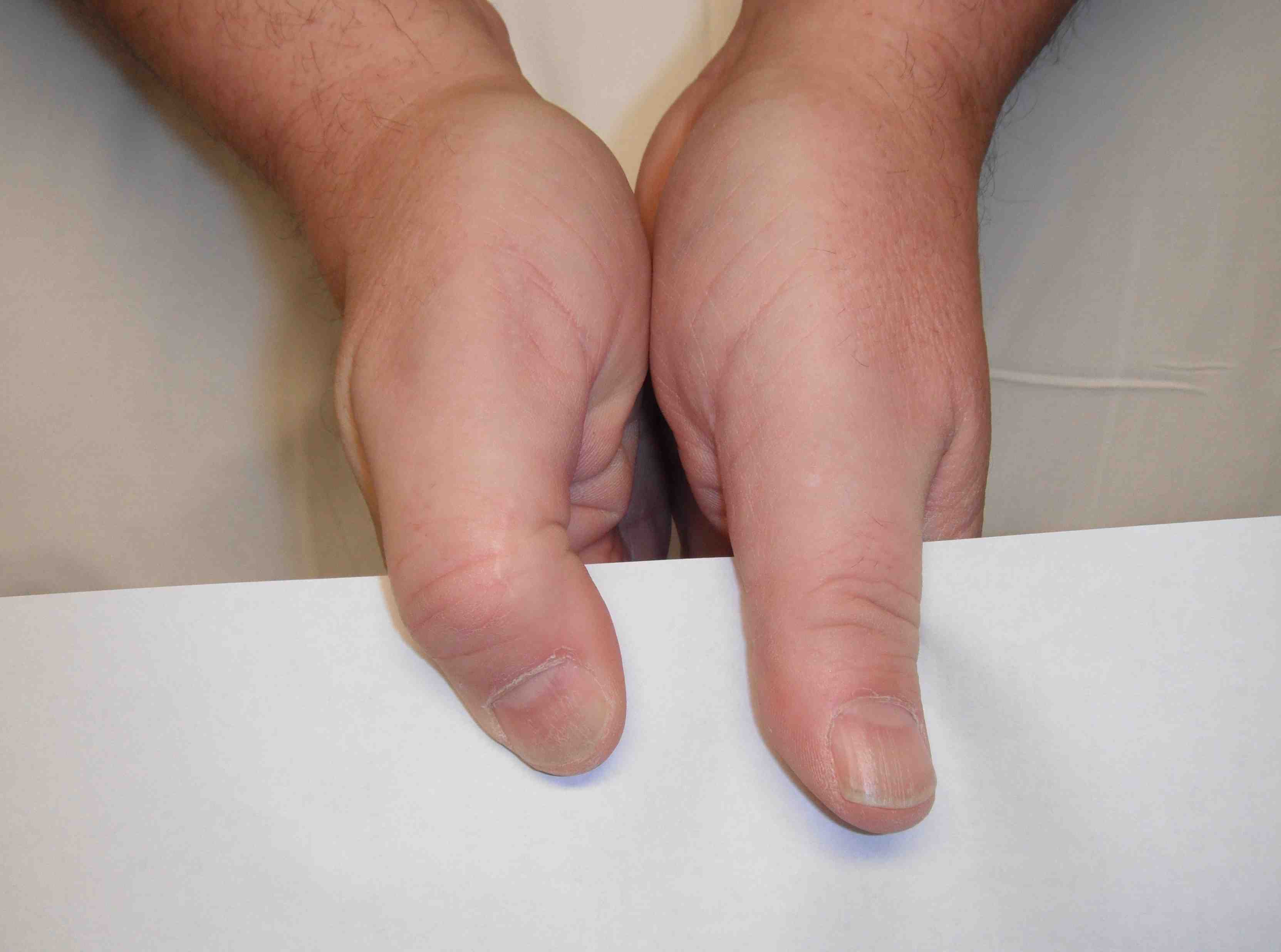
1. Claw hand deformity
Characteristics
- hyperextension all MCPJ
- flexion of IPJ of Ring & Little fingers
A. Absent lumbricals - loss of MCPJ flexion / IPJ extension to RF & LF
2. Unopposed MCPJ extension - EDC
3. IPJ flexed by long flexors - less marked in high lesion because ulnar FDP paralysed
2. Loss of interossei
Weak finger abduction / adduction
Positive Froment's sign
Hypothenar & Interossei wasting
3. Numbness of ulnar 1 & 1/2 fingers
May have numbness of ulnar dorsum of hand
- depends on level of lesion
- if forearm, take out dorsal branch ulna nerve
High Lesion
Above +
A. RF / LF FDP loss
- ulna paradox with less clawing
B. FCU weak
- weak wrist flexion
Goals
1. Restore pinch / thumb stability
- thumb adduction (interposition to BR/ECRB)
- index abduction (EPB to 1st Dorsal Interossei)
2. Correct MCPJ clawing
Management Low Ulna Palsy
1. Thumb adduction
No donor long enough
- FDP LF tendon to BR / ECRB
Technique
- need interposition graft i.e. FDP to LF)
- graft fixed to base P1 / normal insertion
- tendon passed along a line form base of MC III / line of pull of Adductor
- bring out through dorsum between III and IV MC's
- attach to donor tendon BR or ECRB
2. Index Finger abduction
EPB to 1st dorsal interossei
3. Clawing of MCPJ
Goal
Prevent hyperextension of MCPJ's
- Want to create FFD
Options
Static
- Zancolli Capsulodesis / volar plate advancement
Dynamic
- reconstruction lumbricals
- split MF FDS / ECLR into 4
Zancolli Capsulodesis
Transverse palmar incision
- each A1 pulley opened
- flexor tendons retracted
Volar plate raised as distally based flap & advanced proximally
Finger flexed to 20°
- volar plate sutured to new position
- mild FFD MCPJ created
Management High Ulna Palsy
1. FDP to ring and little
Buddy to middle FDP
Problem
- FDP flexes IPJ's before MCPJ's
- this unopposed flexion of IPJ can push object out of palm
2. FCU
Split FCR to FCU