
Indications
Indications have narrowed due to the success of shoulder arthroplasty
1. Chronic infection
2. Obstetric brachial plexus injury
3. Post-traumatic brachial plexus injury
4. Salvage of failed GHJ arthroplasty
5. Arthritic diseases unsuitable for arthroplasty / young patient
6. Tumour resection
7. Instability in epilepsy patients / severe MDI
Contra-Indications
Ipsilateral elbow fusion
Contralateral shoulder arthrodesis
Paralysis of scapula-stabilisers - necessary for function following arthrodesis
Charcot arthropathy (low chance union)
Advantages
Permanent solution
Disadvantages
Loss of movement at shoulder
Difficulty with activities
- at head level or behind the back
- perineal care
Goals
1. Hand should reach
- mouth
- waist
- belt buckle
- back pocket
2. Shoulder be comfortable at rest / scapula should not be prominent
- arm should hang by side with scapula flat against thorax
- no winging
Position
Ideal
- abduction 10-15°
- flexion 10-15°
- internal rotation 45°
Issues
1. Technically difficult to obtain correct position intra-operatively
2. Internal rotation most important to later function
3. Position in reference to trunk not scapula
4. Avoid excessive abduction & flexion
- forces the scapula to rotate & wing at rest
- leads to fatigue & discomfort
Options
Intra-articular
- glenohumeral compression screws +/- acromiohumeral screws
Extra-articular
- plate along spine of scapula / acromion and lateral humerus
Combined
Open Technique

Approach
Midline incision over spine / acromion / down to deltoid tuberosity
A. Posterior
- detach deltoid from spine
- between IS and TM
B. Anterior
- detach deltoid from clavicle
C. Identify and protect axillary nerve
D. Excise rotator cuff tendon
Technique
1. Denude GHJ cartilage
2. Denude superior humeral head and undersurface acromion
3. Temporarily fix with steinman pins GHJ and acromio-humeral
- check position / ROM / no winging
4. Insert GHJ and acromial-humeral compression screws
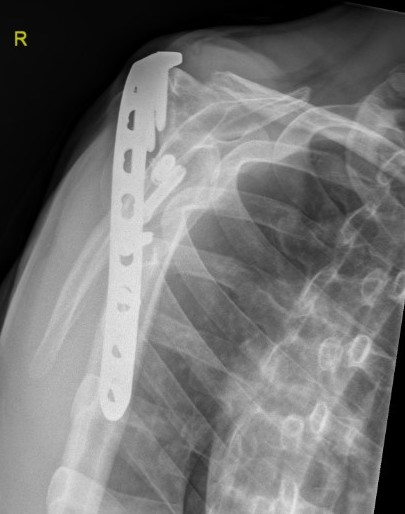
5. Supplement with pelvic reconstruction plate
- 12 - 14 hole
- scapular spine / acromion / humerus
6. Bone graft
7. Careful deltoid repair in case of future conversion to reverse TSR
8. Spica / shoulder abduction sling
Arthroscopic Technique
Complications
Nonunion
Infection
Fracture of humerus below fusion
Prominent hardware
Results
Brachial plexus injury
Atlan et al. J Hand Surg Am 2012
- 54 patients with brachial plexus palsy
- fusion rate 76% after one procedure
- 94% after second operation
- abduction 45 degrees in 75% patients
- rotation 45 degrees in 65% patients
Epilepsy
Thangarajah et al. J Bone Joint 2014
- 6 patients with epilepsy and chronic instability
- all cases achieved union and prevented instability
Failed total shoulder replacement
- 7 patients
- 4/7 required additional procedures to obtain union
- 2/7 persistent non-union
- extremely challenging
Conversion to Reverse TSR
- takedown of 4 patients with scapula pain
- EMG evidence of deltoid function
- some improvements in pain and ROM