

Mechanism of Injuries
Rotational force incurred while joint partially flexed & extending
- caught between femoral & tibial condyles
- usually valgus & ER / varus & IR
Incidence
MM: LM 2:1
Medial Meniscus more common
- less mobile
- usually posterior horn tear
Acute ACL
- lateral Meniscus
Chronic ACL
- medial meniscus
Tibial plateau fracture
- 50% incidence
Relatively common in asymptomatic knees
- 13% < 45 years
- 36% > 45 years
Medial meniscus anatomy
C shaped fibrocartilage
- posterior horn larger than anterior horn
- capsular attachment on the tibial side is the coronary ligament
- thickening of the capsule from tibia to femur is deep MCL

Lateral meniscus
Semicircular
- covers a larger surface of the tibia than MM
- anterior and posterior horns attach closer to each other
- anterior horn adjacent to ACL
- posterior horn behind tibial eminence
- ligaments of Humphrey and Wrisberg are attached to posterior horn
- popliteal hiatus posteriorly
Microstructure
Circumferential type I collagen fibres
- radial fibres to anchor them
- more random mesh structure at surface
- fibrochondrocytes
Blood Supply
Development
- entirely vascular at birth
- inner 1/3 avascular by 1 year
- adult blood supply by 10
Outer 10 - 25% vascular
- genicular arteries
- perimeniscal capillary plexus
Inner 2/3
- nutrition via diffusion
Synovial fringe
- femoral and tibial surface
- does not contribute to the meniscal blood supply
Nerve supply
Similar distribution
- peripheral tears more painful than central tears
- proprioception
Function
1. Transmit and distribute forces over plateau
- load sharing flexion > extension
- shock absorbing
Total medial meniscectomy
- 100% increase in contact stresses
Total lateral meniscectomy
- 200-300% increase in contact stresses
2. Secondary stabilisers
- posterior horn resists anterior translation in flexion
- important in ACL deficient knee
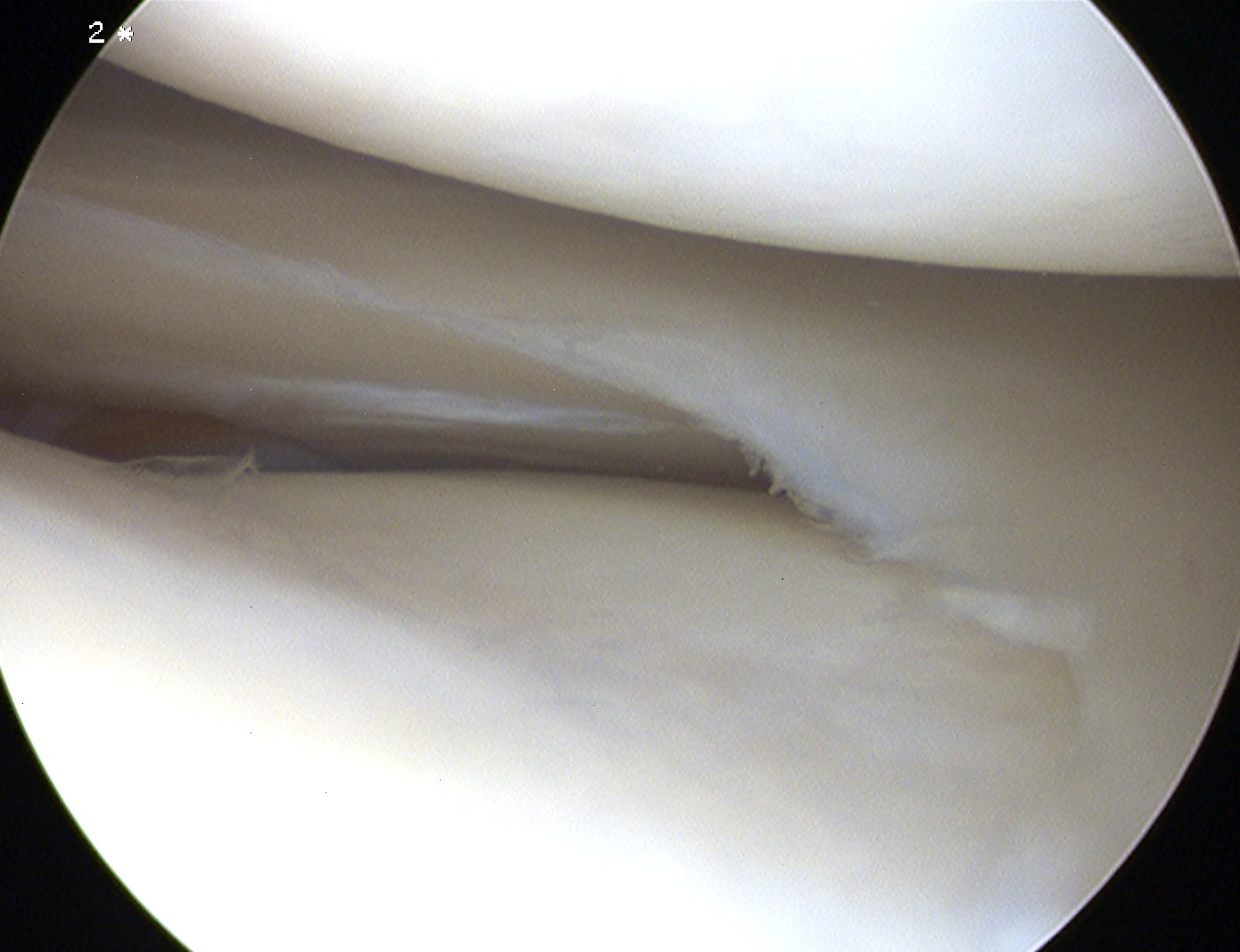
Classification
1. Longitudinal Tears
Most common
- vertically oriented tear parallel to edge of meniscus
- usually of posterior part of meniscus
- may occur in either meniscus
- extent varies
A. Incomplete
- usually inferior surface
- may have been complete then healed
- very common posterior horn lateral meniscus after ACL rupture
B. Complete
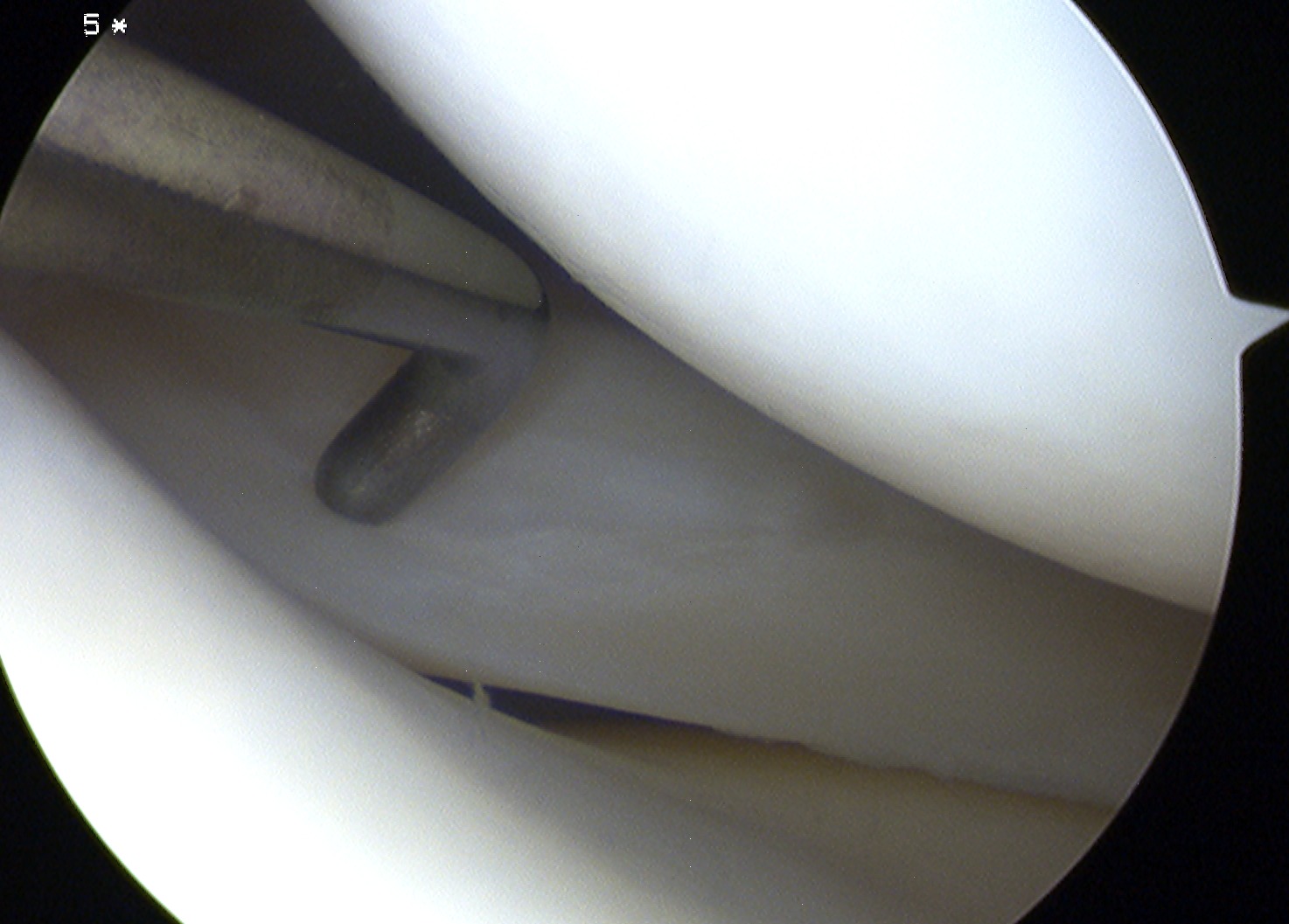
C. Bucket handle
- displaces into intercondylar notch
- may be central or peripheral
- cause of locked knee
- can damage chondral surface over time
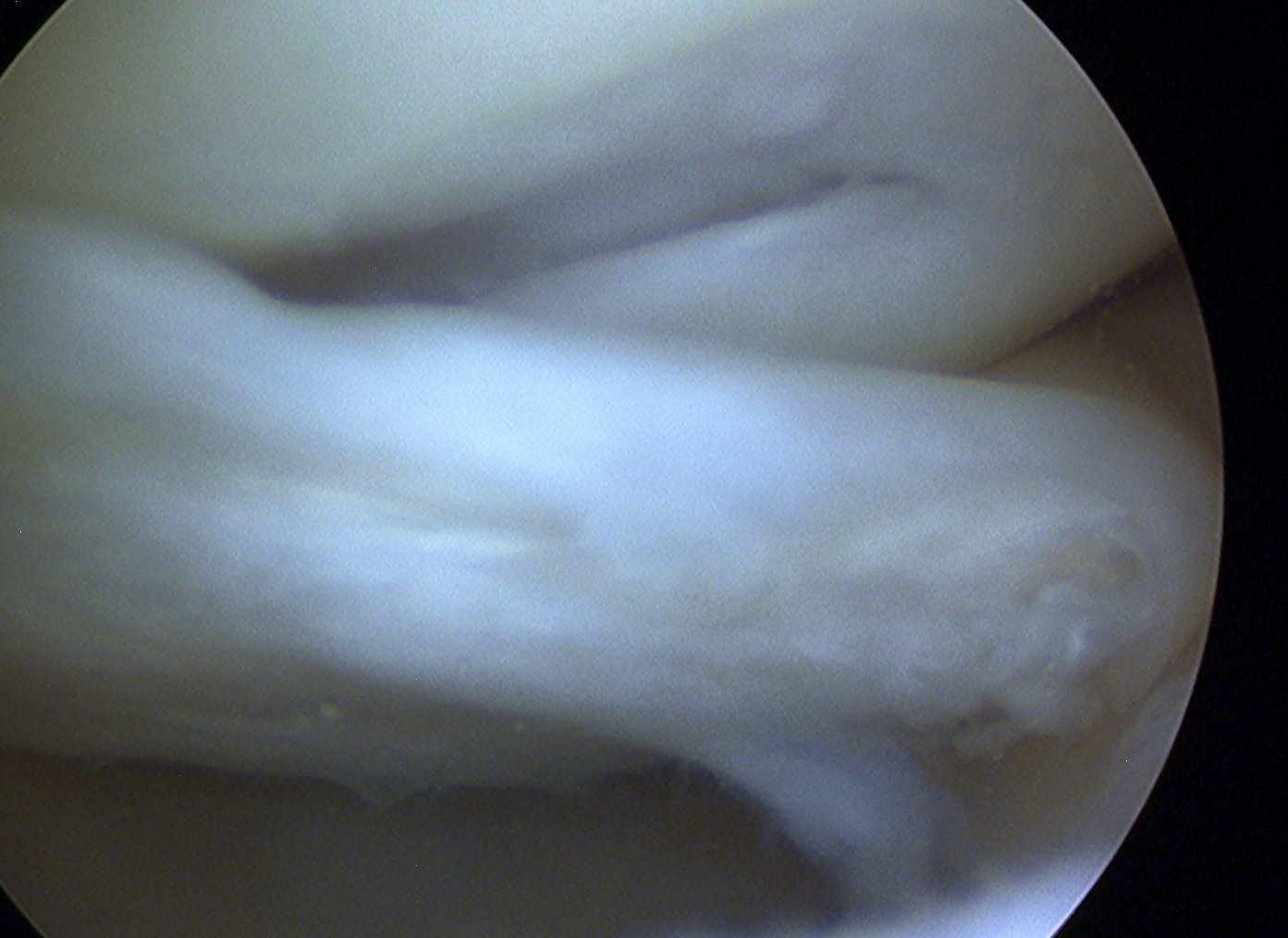
2. Horizontal Cleavage
More common in older patient
- horizontal cleavage plane between superior & inferior surfaces of meniscus
- posterior 1/2 of MM
- mid-segment of LM
3. Oblique
Vertically oriented full-thickness tear
- runs obliquely from inner edge of meniscus out to body of meniscus
- if base posterior, referred to as posterior oblique tear & vice versa
4. Radial
Vertically oriented full thickness tear
- extends from inner edge radially to periphery
Incomplete
- doesn't extend to periphery
Complete
- extends to periphery
Parrot beak tear
- incomplete radial tear with anterior or posterior extension
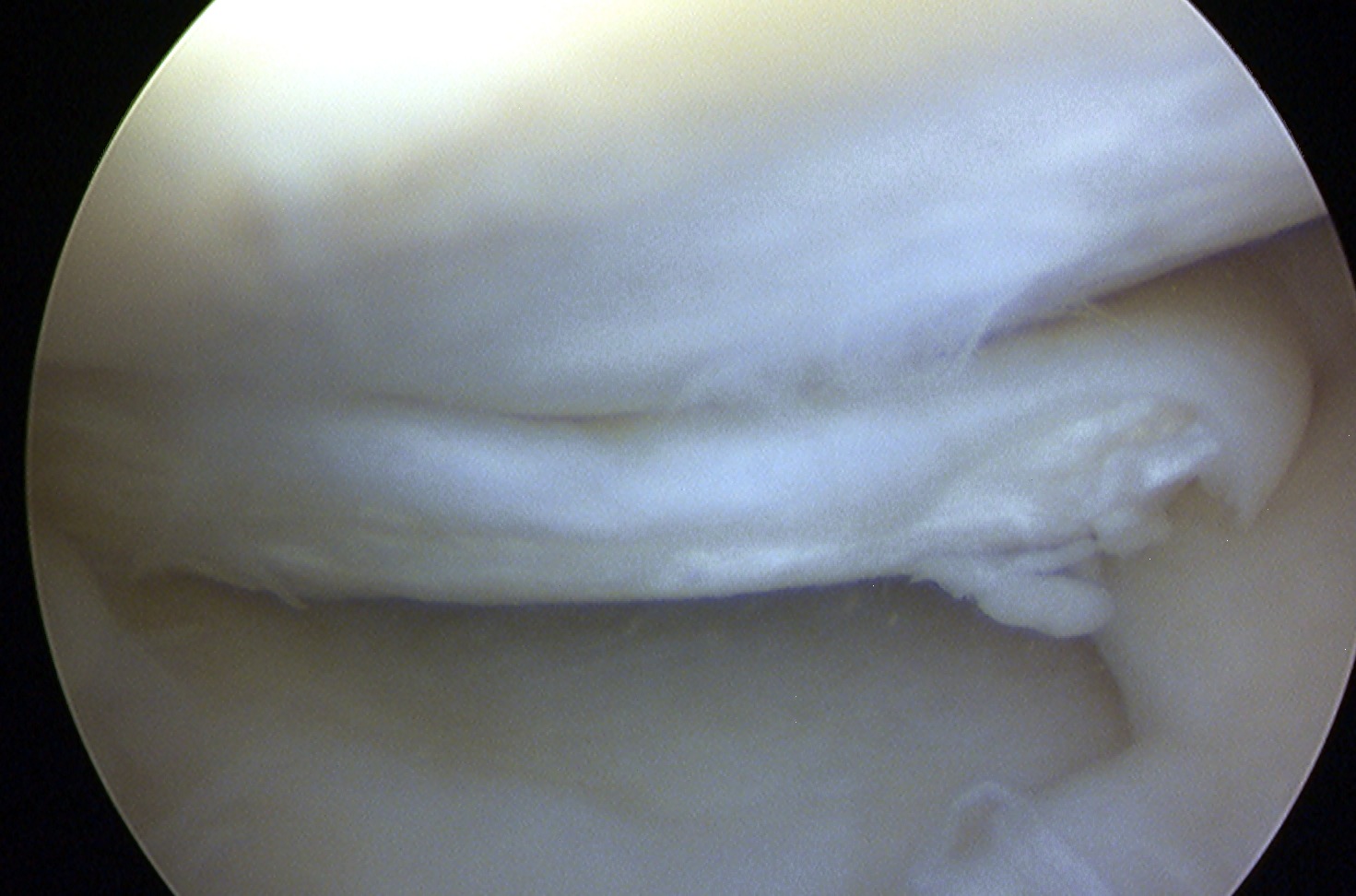
5. Complex
Elements of all above
- usually in longstanding meniscal lesions
6. Degenerative
Complex tear of degenerative meniscus / usually OA

Blood Supply Classification
Red - Red Tears
- peripheral 3 mm
- capsulomeniscal junction
- good blood supply
- both sides vascularised
Red - White Tears
- only one side of tear vascularised
White - White Tears
- peripheral
- neither side vascularised
Symptoms
History of injury
- twist with weight bearing
- may not be a specific injury especially in middle-aged patient
Swelling usually delayed 6 hours & mild
- can be chronic from synovial irritation
- may be rapid haemarthrosis with capsular tear
Locking
- only with longitudinal tears / bucket handle tear
Giving Way
- may occur with other knee disorders
- i.e. loose body, instability, weak quadriceps
Signs
Effusion
Tenderness
- along periphery of meniscus
- along joint line
- pain secondary to synovitis in adjacent capsule
McMurray's Test
- tests menisci posterior to collateral ligaments
- point heel towards meniscus testing
- positive test is palpable or audible snap or click
1. Fully flex knee
2. Place leg into full IR -> tests LM
3. Extend to 90°
4. Place leg into full ER -> tests MM
5. Extend to 90°
X-ray
Standard Knee Series
Exclude SONK / loose bodies / OCD / tumour
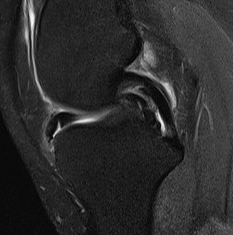
MRI Classification
Stoller 1987 J. Radiol.
Grade 0
- normal homogeneous low signal intensity
Grade I
- globular increase signal in meniscus
- doesn't reach either surface
Grade II
- linear increase signal, doesn't reach surface
- myxoid intra-meniscal degeneration / partially healed tear

Grade III
- increased signal intensity communicates with meniscal surface
- 70-90% accurate for true tear
- accuracy MM > LM
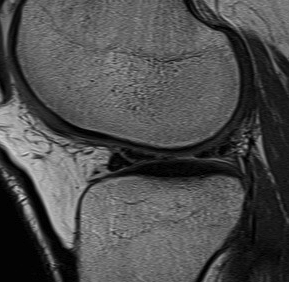
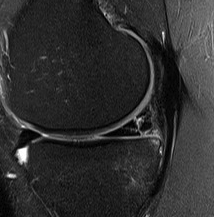
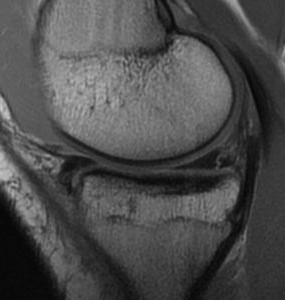
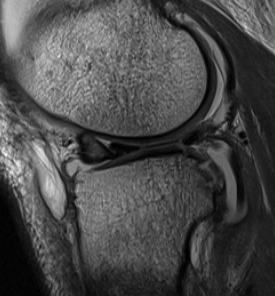
MRI Pitfalls / Normal Findings or Variants
Ligaments of Wrisberg PMFL & Humphrey AMFL

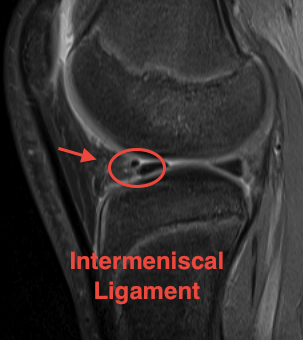
Transverse Anterior Meniscal Ligament
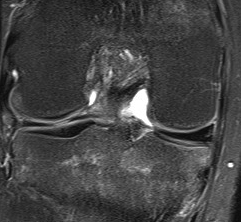
Signs of bucket handle tear meniscus
1. Double PCL sign
- medial Meniscus

2. Absent bow tie sign
- should see bow tie image on 2 consecutive sagittal slices of 5 mm
3. Fragment in notch sign

4. Anterior flipped meniscal sign
- torn fragment flips over the anterior horn of the affected meniscus
5. Truncated meniscus
Arthroscopy
Mainstay of diagnosis and treatment
Bone Scan
Don't forget SONK in differential
- 60 yr old female with normal x-rays
- acute onset pain
- AVN MFC
Should usually show up on MRI
Management
Surgical Indications
Painful locking / clicking with disability
Acutely locked knee
Repairable meniscus in combination with ACL injury
Repairable meniscal injury in young
Options
1. Leave / non operative treatment
2. Excise
3. Repair
4. Meniscal transplant
Non Operative Treatment
Essentially the asymptomatic patient
A. Stable partial thickness (< 50%)
B. Stable longitudinal < 1 cm long
C. Small < 3 mm radial tears
ROM exercises + quads drill