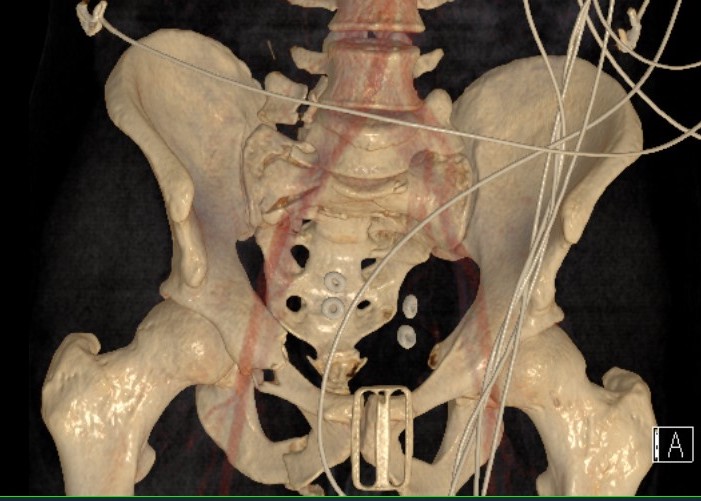
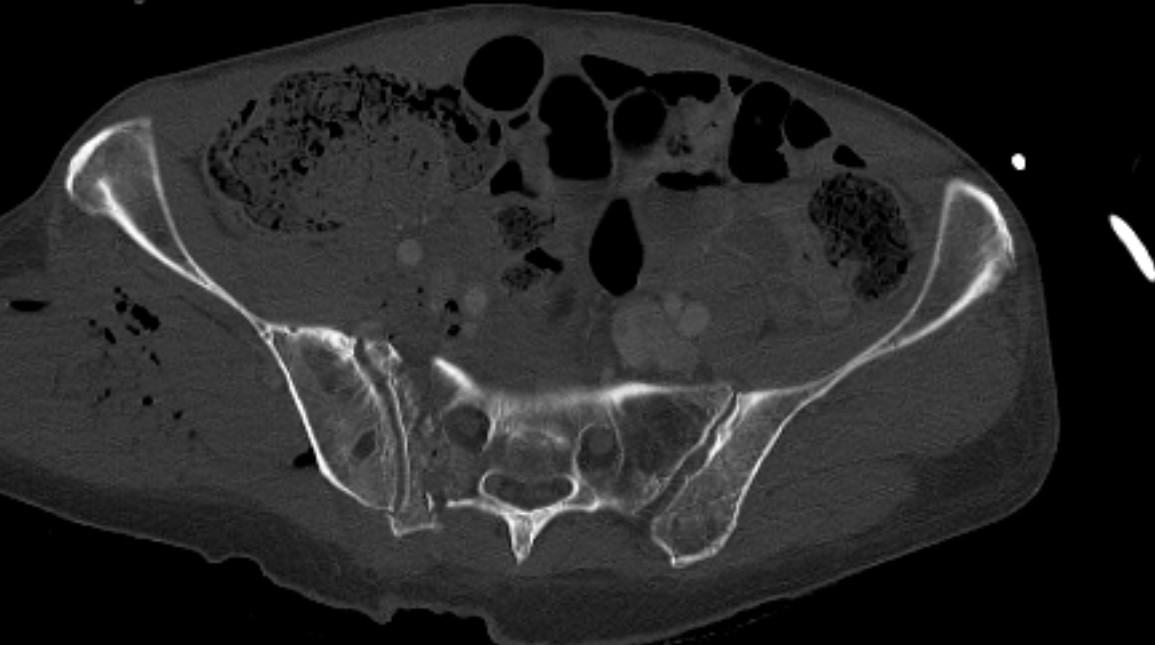
LC-1: pubic rami fracture with sacral fracture
Non operative management
Beckmann et al J Orthop Trauma 2014
- 27 cases of LC-1 presented to 111 trauma surgeons
- only 9/27 (33%) of cases had substantial agreement on management plan
Indications
< 1 cm displacement
Stable
- incomplete sacral fractures
- no pubic rami fractures
- < 10 mm displacement on lateral stress xray or EUA
Stability
Indications for EUA / lateral stress xray
- complete sacral fracture with pubic rami fractures
- internal rotation force
- look for displacement of pubic rami fractures
- EUA of 20 LC-1 fractures
- 35% deemed unstable requiring surgery
Parry et al J Orthop Trauma 2020
- lateral stress xray with patient in lateral decubitus
- correlates with examination under anesthesia
Results
- systematic review of operative versus non operative treatment of unstable LC-1
- all with complete sacral fractures
- 183 surgical and 314 non surgical patients
- surgical patients had lower pain levels
- surgical patients had better quality of life, but non significant
Gaski et al J Orthop Trauma 2014
- retrospective review of 50 patients with LC-1 fractures treated non operatively
- all had complete sacral fractures with < 10 mm displacement
- 35/37 patients without other injuries had a good or excellent outcome
Soles et al J Orthop Trauma 2012
- 118 patients with LC-1 complete sacral fracture < 10 mm displacement
- all allowed immediate weight bearing
- 1 patient had significant pain and xray signs of displacement at 1 week requiring fixation
Operative management
Indications
> 10 mm displacement
EUA / lateral stress view
- complete sacral fracture with instability
Technique
Posterior fixation
EUA
Anterior fixation if unstable or bilateral pubic rami fractures
Results posterior +/- anterior fixation
- 227 patients with LC fractures
- those with oblique or comminuted fractures of the superior and inferior pubic rami more likely to be unstable on EUA
- 11/11 of these treated with posterior only fixation underwent further displacement
- 74 patients with LC fractures
- EUA following posterior fixation determined need for anterior fixation
- patients with posterior fixation and unilateral rami fractures united without further displacement
- patients with bilateral superior and inferior pubic rami treated without anterior fixation underwent further displacement
Posterior fixation
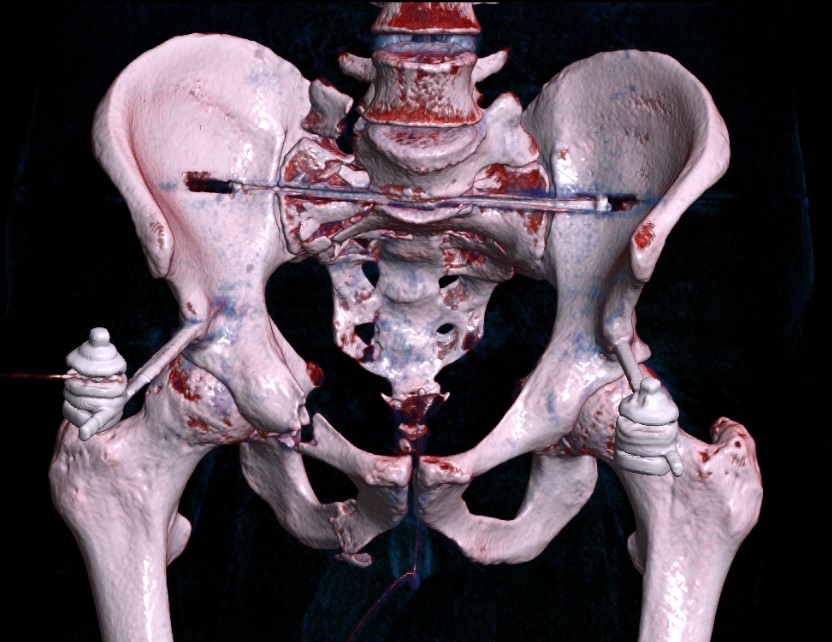
Percutaneous sacroiliac screws
Posterior approach + / - plates
- highly comminuted
- reduction
Percutaneous sacroiliac screws
Vumedi video percutaneous SI screws
AO surgery reference percutaneous SI screw

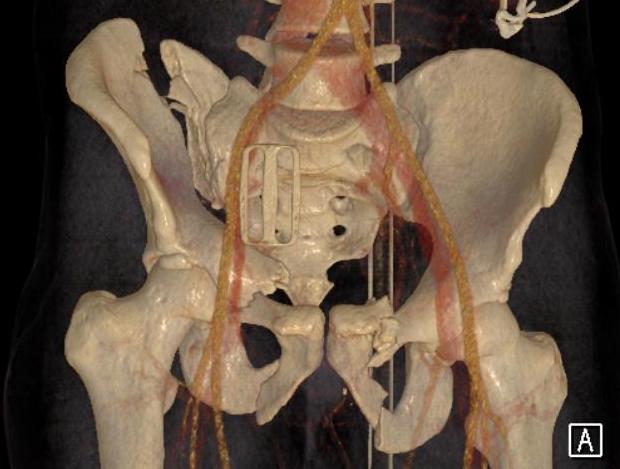
Posterior sacral plates
Technique
- patient prone
- vertical incision 1 cm lateral to PSIS
- from crest to sciatic notch
- incise and reflect G maximus
- apply transverse plate
- soft tissue can be a problem
Anterior fixation
Indications
- instability following posterior fixation
- bilateral pubic rami fractures
Options
- plate - modified stoppa
- percutaneous ramus screws
- external fixation


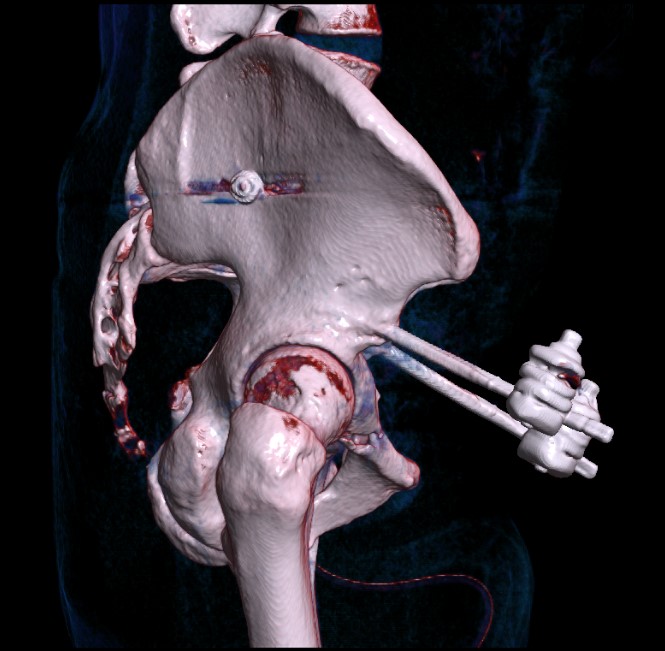
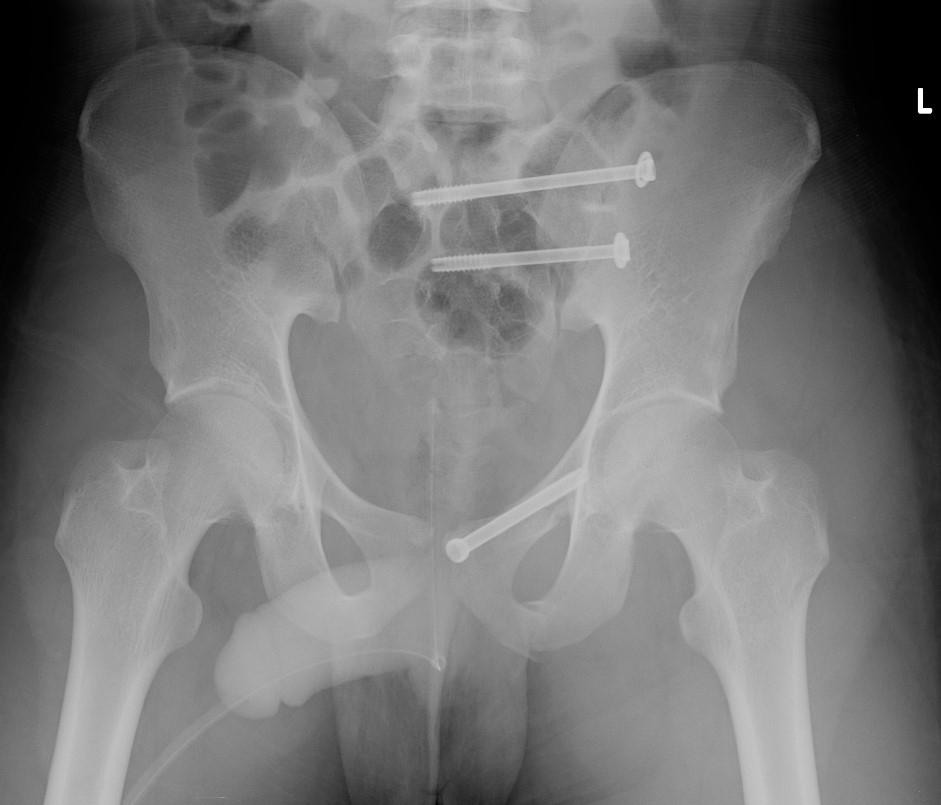
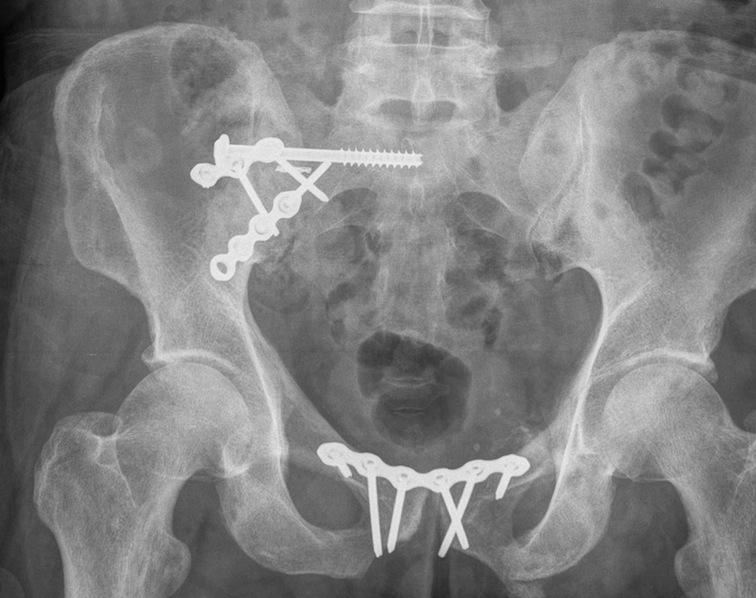
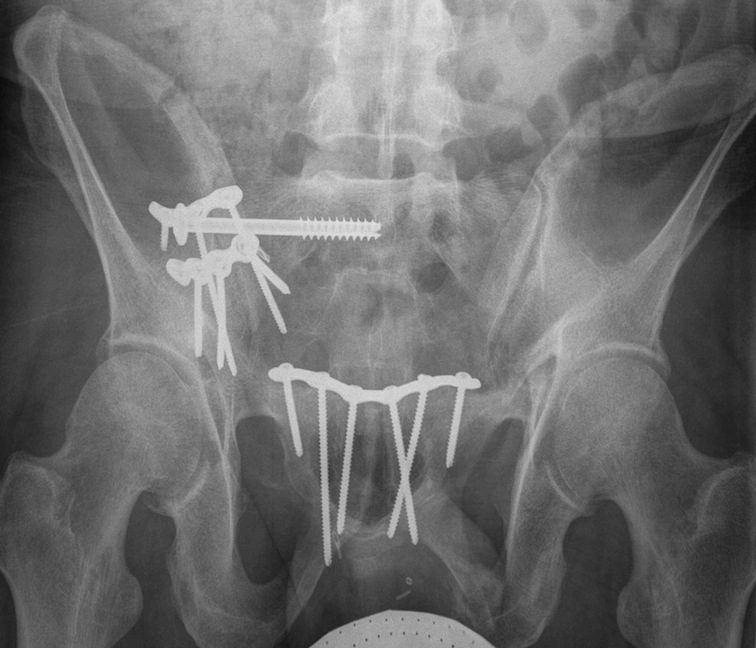
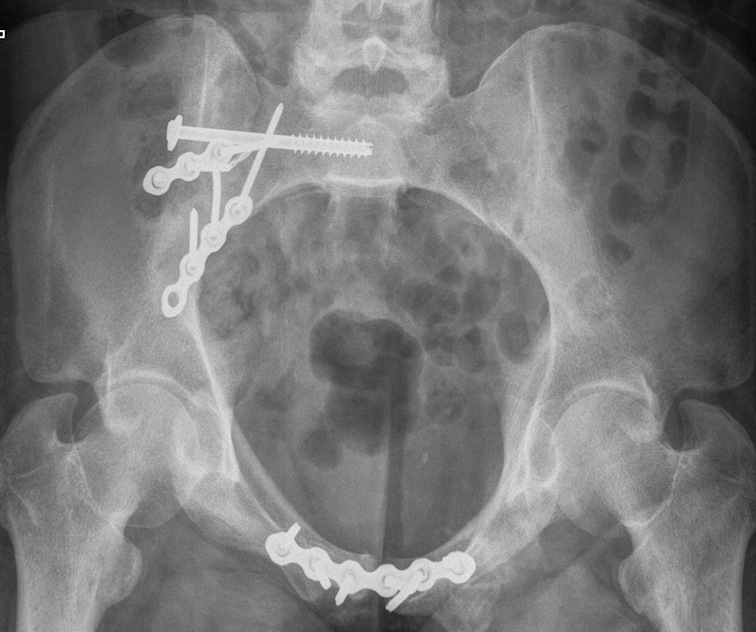
LC-1 with anterior external fixation Plating of bilateral pubic rami fractures
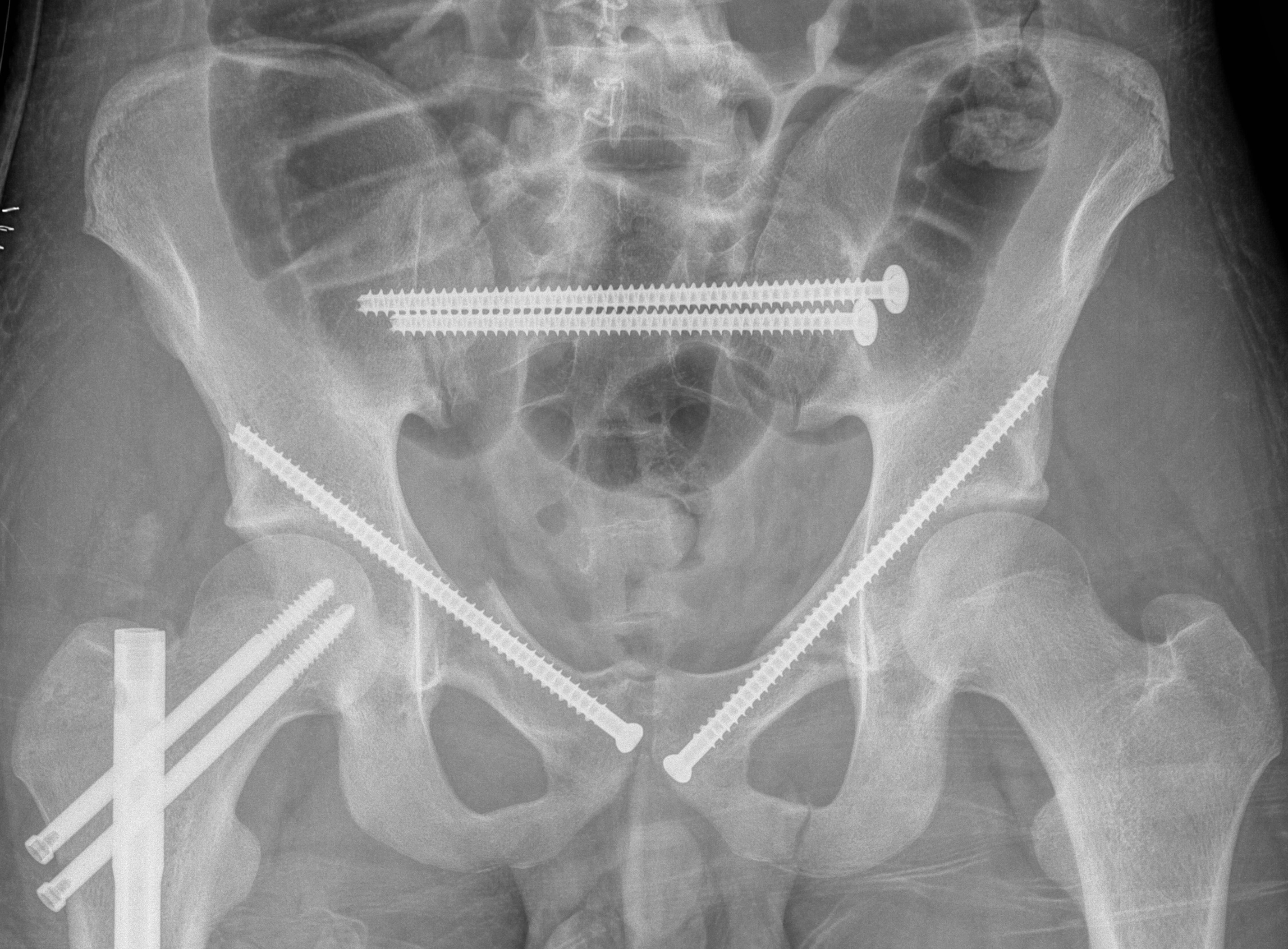
Percutaneous ramus screw
Vumedi pubic rami screw and IM nail
AO surgery reference pubic rami screw
AO surgery reference pubic rami plate
LC-2: Pelvic wing fracture with pubic rami fracture
Crescent fracture variant
Iliac wing fracture that extends into sacrum and associated with SI joint dislocation
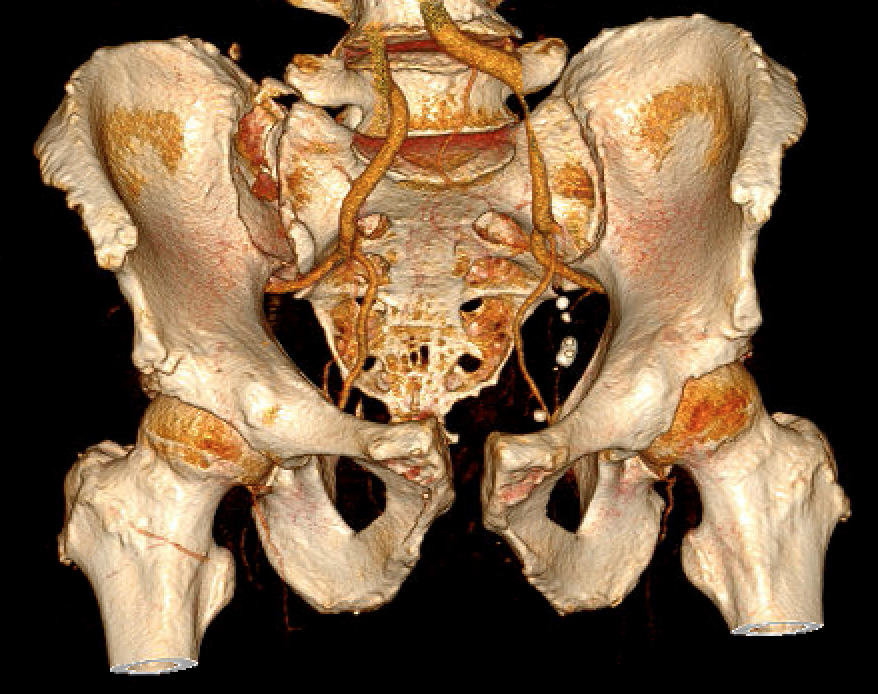


Crescent fracture
Non operative management
Indications
< 10 mm displacement
Stable
Results
- 78 LC-2 with < 10 mm displacement treated nonoperatively
- 45 LC-2 with > 10 mm displacement treated operatively
- no difference in pain scores
Operative management
Options
Posterior fixation - iliac plates
Anterior fixation
- plate / percutaneous screws / external fixation
Anterior versus posterior fixation versus both
- retrospective review of LC-2 fractures
- 44 underwent posterior fixation alone
- 49 underwent anterior and posterior fixation
- increased blood loss and transfusion in AP fixation
- no differences in time to weight bearing, time to union, or functional outcome
Iliac fracture plating
Technique
- use lateral window of ilioinguinal approach
AO surgery reference ilioinguinal approach
Outcomes of Lateral Compression Fractures
Hammad et al Orthop Traumatol Rehab 2021
- compared 21 surgically treated LC-1 to 16 surgically treated LC-2
- better outcomes and increased return to work in those with iliac fractures compared to sacral fractures
- 119 patients with unstable LC fractures treated surgically
- persistent disability the norm
- complicated by high rate of other significant lower limb injuries