Options
Direct Lateral - transgluteal
Postero-lateral (AKA posterior) - release short external rotators
Direct Anterior
Results
Gait / outcomes
Meermans et al Bone Joint J 2017
- systematic review of 42 studies comparing Direct Anterior / Posterior / Lateral
- better outcomes in Direct Anterior in first 6 weeks
- no difference in outcome scores after 6 weeks
- no difference in three approaches on gait analysis or length of stay
Peng et al BMC Musculoskeletal Disorders 2020
- meta-analysis of 7 RCTS and 600 patients
- Direct Anterior versus Posterior
- reduced pain and improved function with Direct Anterior at 6 weeks
- no difference at 3,6 or 12 months
Dislocation
Koster et al J Orthop Trauma Rehab 2023
- meta-analysis of 11 studies and 2,000 patients
- dislocation rates
- posterolateral 1.4% / anterior 0.4% / lateral 0%
Steenbergen et al Hip Int 2023
- Dutch registry of 270,000 THA
- posterior 1.4% / anterior 0.4% / lateral 0.6%
Revision
Australian Joint Registry 2023 7 years % revision
| Anterior | Posterior | Lateral | |
|---|---|---|---|
| Revision overall | 3.1 | 3.3 | 3.5 |
| Revision for loosening | 1.0 | 0.4 | 0.6 |
| Revision for fracture | 0.8 | 0.7 | 0.6 |
| Revision for infection | 0.6 | 1.0 | 1.0 |
| Revision for dislocation | 0.3 | 0.9 | 0.8 |
Direct Anterior
Advantages
- muscle sparing - early mobilization in first 6 - 12 weeks
- ease of intra-operative image for component position
Disadvantage
- learning curve
- LFCN injury
- femoral nerve injury with anterior retractor
- femoral exposure more difficult / risk of intra-operative fracture
Complications
- meta-analysis of Anterior versus Lateral approach
- 13 studies and 25,000 THA
- reduced prosthesis malposition / LLD / Trendelenberg gait with anterior approach
- increased dislocation / periprosthetic fracture / loosening with anterior approach
Technique
AO Surgery Reference Direct Anterior
Smith-Petersen Approach
- supine +/- traction table
- vertical incision from ASIS over TFL
- identify and protect LFCN
- develop plane between TFL and sartorius
- identify and coagulate lateral femoral circumflex vessels
- plane between rectus femoris and gluteus medius
- femoral osteotomy and remove head
Acetabulum
- externally rotate leg
- check position with intra-operative images
Femur
- extension / adduction / external rotation
- use bone hook to elevate femur
- check offset with intra-operative images
Direct Lateral / Hardinge
Advantage
- reduced dislocation rate
Disadvantage
- divide abductors - abductor weakness / Trendelenberg gait
Complications
- RCT of direct lateral versus anterior THA in 160 patients
- incidence trendelenberg gait at 2 years
- 16% with direct lateral
- 1% with direct anterior
Technique
AO Surgery Reference Direct Lateral
Hardinge approach
- patient in lateral decubitus
- incision centered on greater trochanter
- split fascia and gluteus maximus
- release anterior 1/3 of gluteus medius and gluteus minimus
- limit superior muscle split to protect superior gluteal nerve
- release anterior vastus lateralis and cauterize ascending medial circumflex
- T capsulotomy
- dislocate femoral head by external rotation
- place foot in foot bag
Postero-lateral
Disadvantage
- ? increased dislocation rate
Complications
Dimentberg et al Arch Orthop Trauma Surg 2023
- 2,200 THA with posterior approach
- 1% dislocation rate with tendon to bone short external rotator repair
Anderson et al J Arthroplasty 2023
- 2,900 THA with posterior approach and guidance
- 0.4% dislocation rate
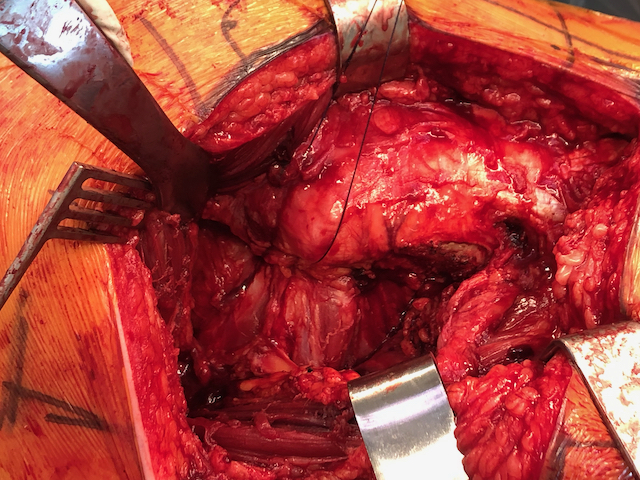
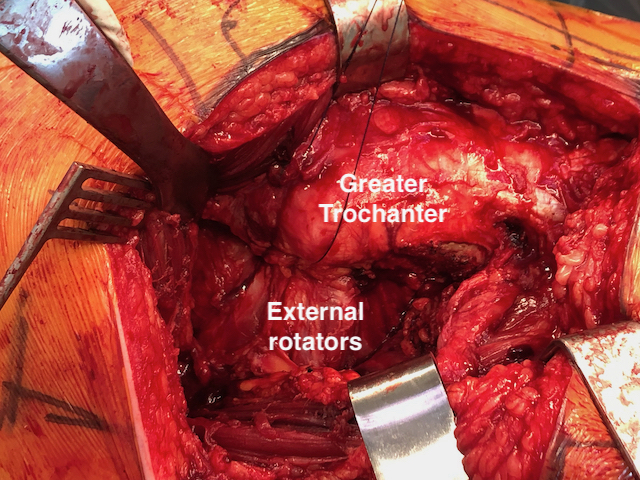
Technique
AO Surgery Reference Posterior Approach
Vumedi Posterior Approach video
- lateral decubitus
- incision centered on greater trochanter
- split fascia
- identify short external rotators
- open interval between G medius and piriformis
- place stay sutures in short external rotators and release insertion
- open capsule
- dislocate hip via internal rotation