
Definition
Bilateral pars fracture of C2
Traumatic spondylolisthesis of C2
Mechanism
Motor vehicle accident
Fall from height
Neurological injury
Neurological injury thought to be uncommon as fragments separate and decompress
Different to judicial hanging where spinal cord is severed
Gangzhou et al J Orthop Res 2017
- 97 patients with hangman's fracture
- 23/97 with neurological injury
- all partial spinal cord injuries
- associated with increased displacement / angulation (type II, IIa, III)
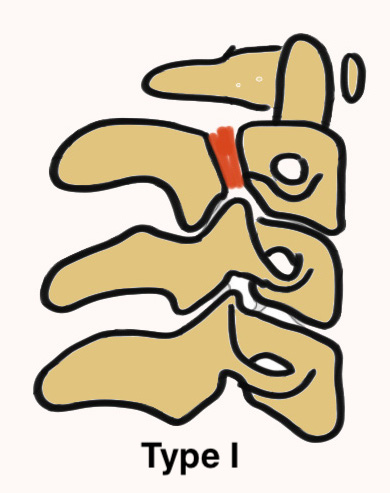
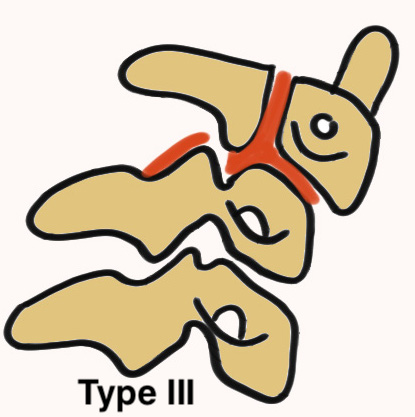
Levine & Irving Classification
| Type | Characteristics | Mechanism | Management |
|---|---|---|---|
| Type I |
Vertical fracture line < 3 mm anterior displacement C2/3 disc normal |
Axial compression and hyperextension | Collar 6 weeks |
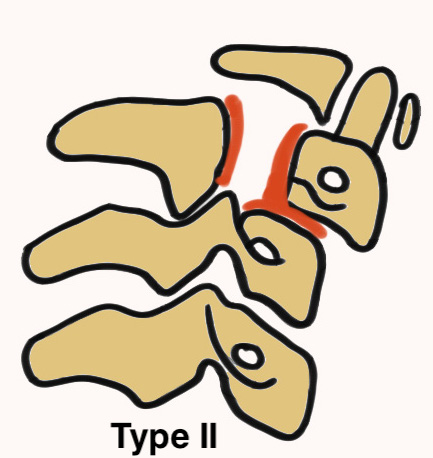
| Type II |
Vertical fracture line > 3 mm anterior displacement C2/3 disc disrupted Unstable |
Axial compression and hyperextension |
Traction and halo-vest Consider surgery |
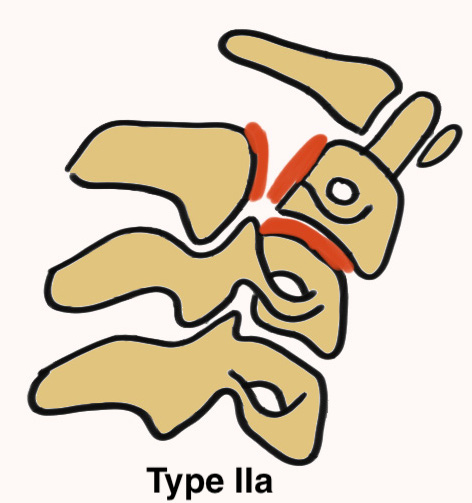
| Type IIa |
Horizontal fracture line Significant angulation
|
Flexion-distraction |
Avoid traction Hyperextension and halo-vest Consider surgery |
| Type III | Type I with C2/3 facet dislocation | Surgery |
Murphy et al J Orthop Trauma 2017
- 548 fractures mean age 38
- Type I: 46/548 (8.4%)
- Type II: 228/548 (41.6%)
- Type IIa 89/548 (16.2%)
- Type III: 35/548 (6.4%)
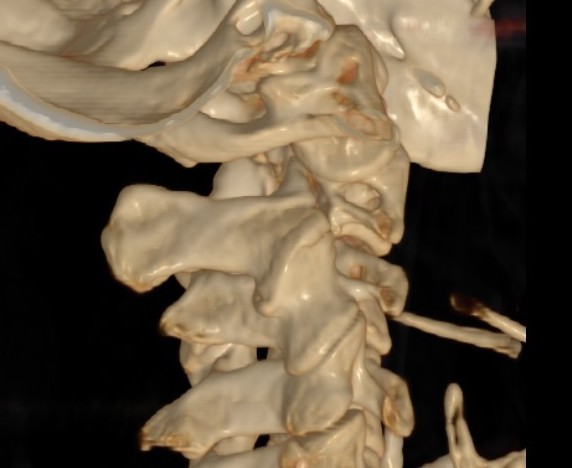
Xray



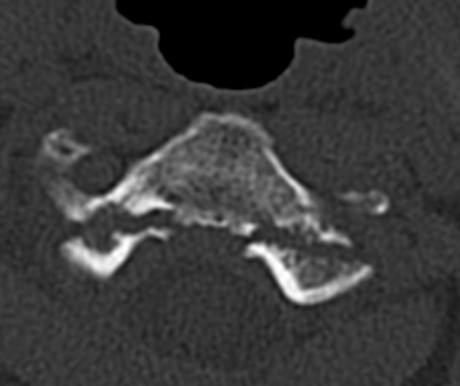
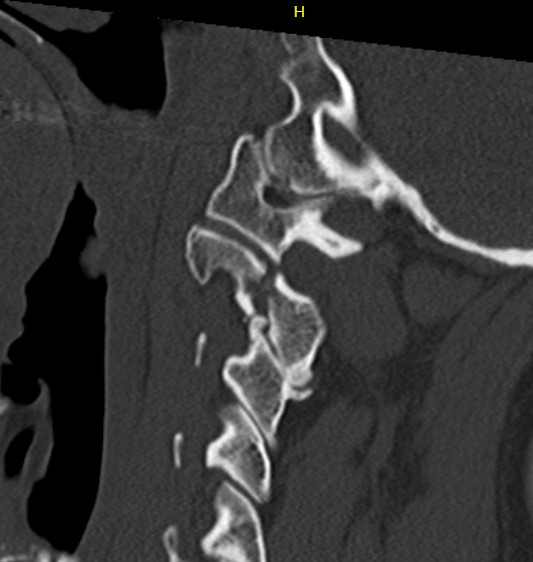
CT scan



Management
Instability
Disruption of C2/3 disc and posterior longitudinal ligament (PLL)
- significant anterior displacement (Type II)
- significant angulation (Type IIa)
- Type III
Nonoperative management
Indication
Type I
- collar 8 weeks
- flexion extension views to assess stability
Results
Murphy et al J Orthop Trauma 2017
- systematic review of operative versus nonoperative care
- union rate of 131 fractures treated nonoperatively was 94%
- union rate of 417 fractures treated operatively was 99%
- systematic review
- union rates with nonoperative management
- Type I: 100%
- Type II: 60%
- Type III: < 40%


Hangman's fracture reduced and held in halo-vest


Post halo flexion and extension views demonstrating fracture stability
Operative Management
Indications
Significant displacement / angulation with disc and PLL damage
- Type II
- Type IIa
- Type III
Options
Anterior fixation / fusion
Posterior fixation / fusion
Combined
Anterior
Anterior cervical discectomy and fusion ACDF
ACDF C2/3
- preserves C1 motion
- lower risk of vertebral artery injury
Zhonghai et al J Neurosurg Spine 2015
- 38 patients with unstable hangman's fracture
- treated with ACDF or C3 corpectomy and fusion
- fusion in 36/38 (95%)
Posterior
1. Posterior C1 - C3 fusion
Significant loss of motion
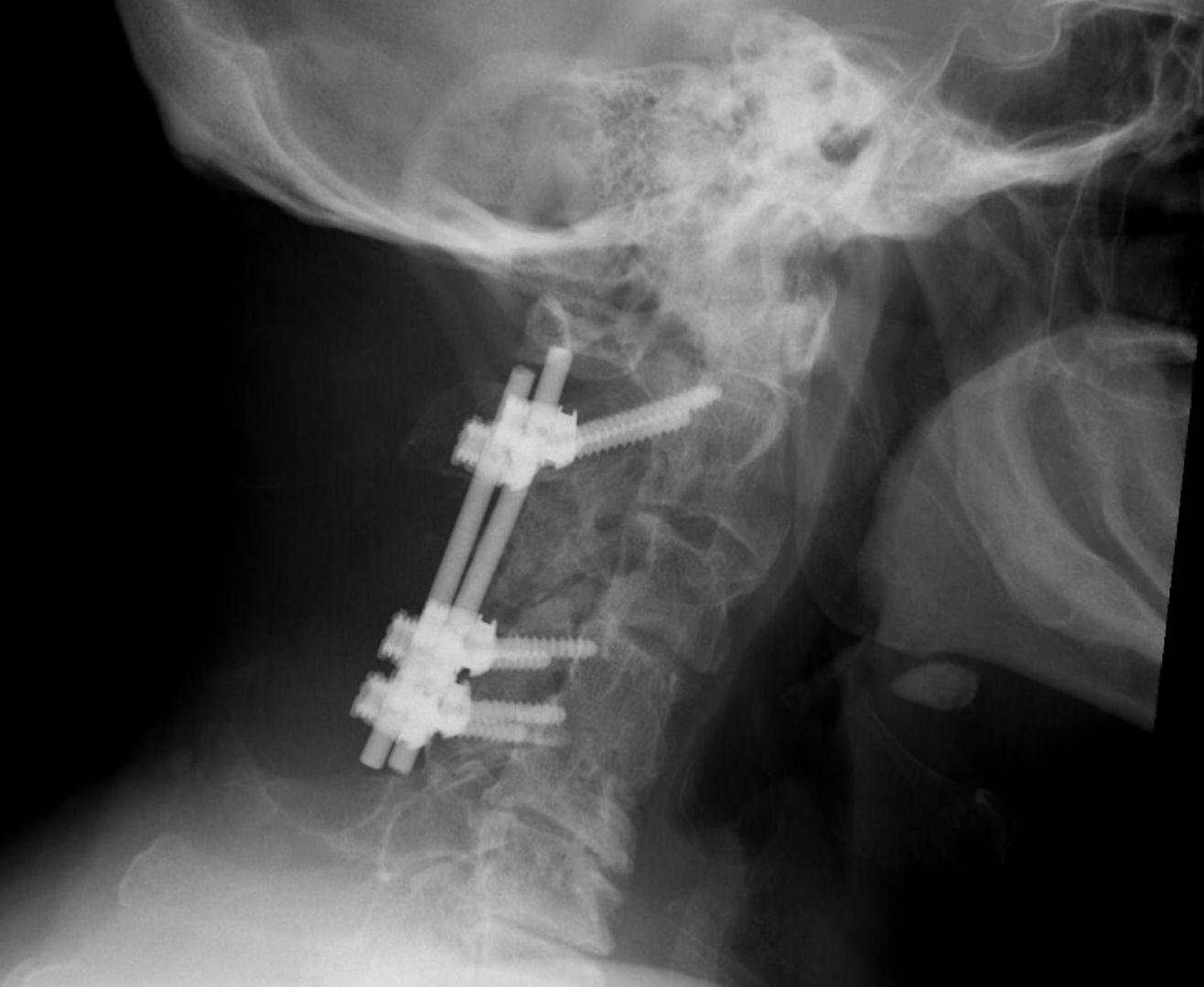
2. C2 trans-pedicle screw fixation + C3 fixation +/- fusion
Short segment fixation +/- fusion
- preserves ROM
- 35 unstable C2 hangman's fractures
- C2 / C3 posterior short segment fixation and fusion
- 100% fusion at 6 months in all cases
3. C2 trans-pedicle lag screw fixation
Liu et al J Orthop Surg Res 2020
- 25 patients with unstable C2 hangman's fractures
- reduced with tongs
- fixed with transpedicle screws
- 100% osseous union and full range of motion