
Epidemiology
High energy trauma
Usually deadly
Zivot et al Am J Forensic Med Pathol 1993
- autopsies of 85 fatal pedestrian - MVA accidents
- 31% had atlanto occipital dislocation
- death likely due to brainstem injury
Children
More common in children due to
- larger head to body ratio
- relative ligamentous laxity
- horizontal atlanto-occipital joints
Types
Pure ligament injury usually
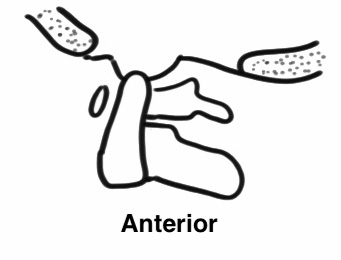
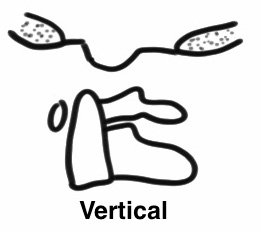
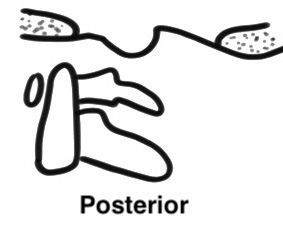
Direction
- anterior occipital displacement (most common / head anterior)
- vertical
- posterior (rare)
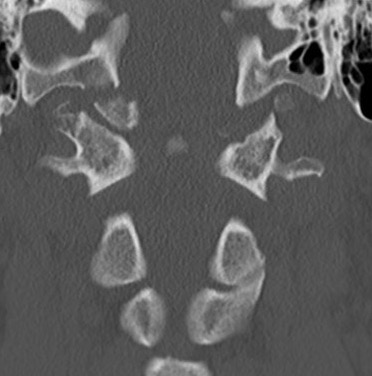
Xray / CT measurements
Frequently missed on xray

Basion-Dens Interval / BDI
- basion to tip of dens
- vertical displacement > 12 mm
Basion-Axial Interval / BAI
- basion to posterior border ondontoid
- anterior displacement > 4 mm
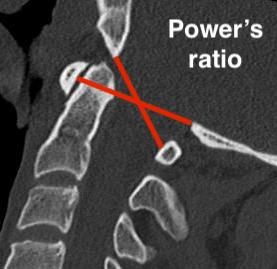
Power Ratio BC/AO > 1
- basion to posterior arch / opisthion to anterior arch

From: Kim et al Korean Journal of Spine 2012
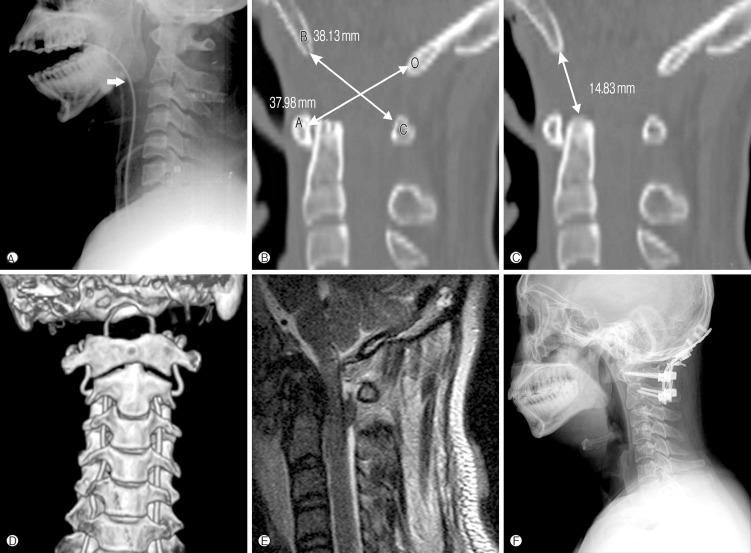
From: Kim et al Korean Journal of Spine 2012
Management
Outcomes
Joaquim et al Int J Spine Surg 2021
- systematic review of 17 articles and 341 patients who survived to hospital
- mortality rate 35%
- mean GCS 8
- high incidence of cardiac arrest
- high association of intra-cranial injury
- 11% severe neurological injury
- majority survivors treated with occipito-cervical fusion
Reduction and Halo-Thoracic Brace (HTB)
Reduce in OT
- image intensifier
- putting sandbags under thorax
- allows head to reduce posteriorly
- assess with image intensifier
- apply halo vest
- add compression
HTB 3 months
- assess stabilty with flexion / extension views
Surgical stabilization
Occipito-cervical fusion