Indications
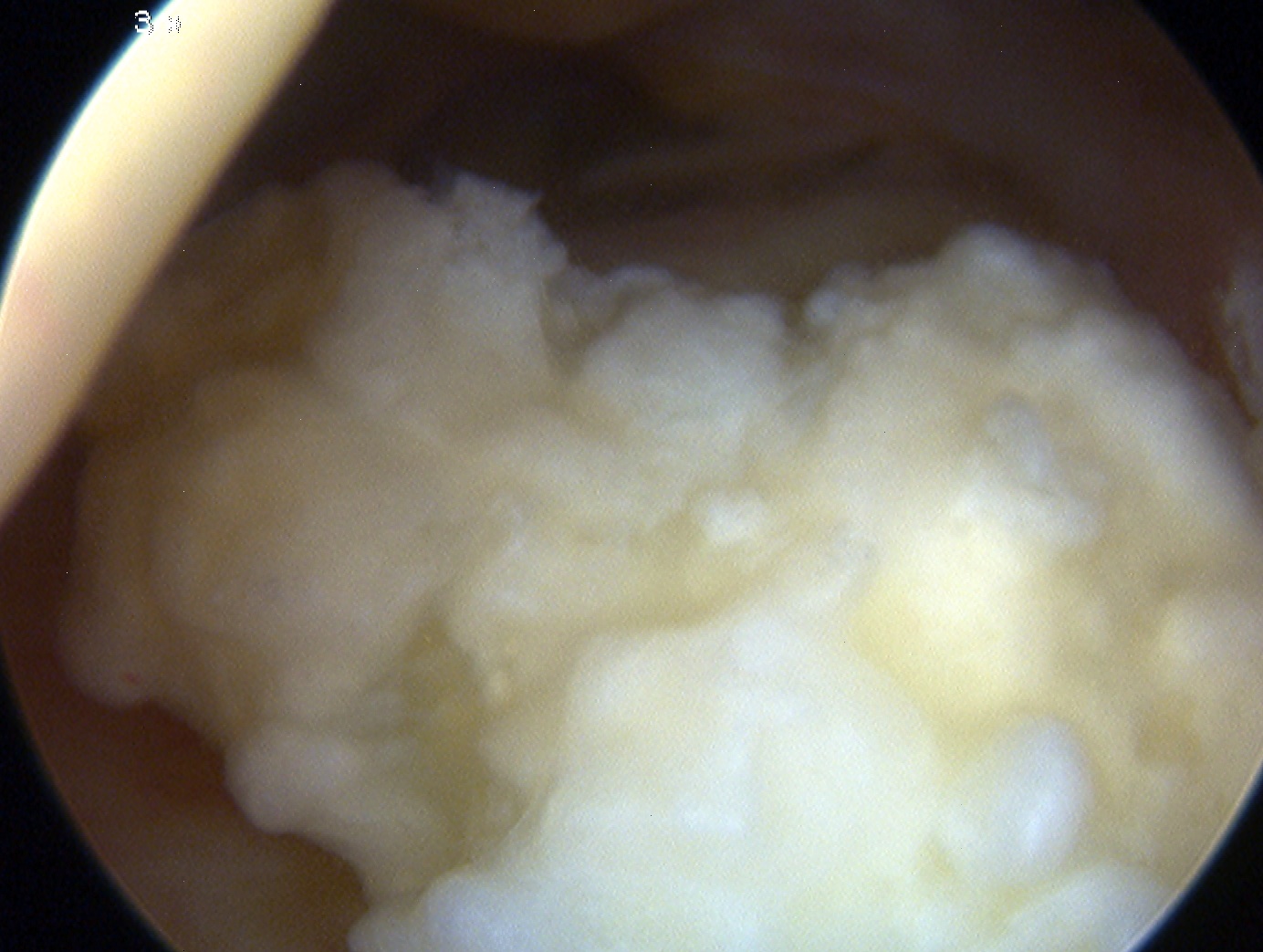
1. Removal Loose body
2. Excison of osteophytes
- coronoid
- olecranon
- aiming to improve ROM / prevent impingement
3. Elbow Stiffness Capsular Release
- capsular contraction can limit range
- anterior capsulotomy
- risk to median nerve anteriorly
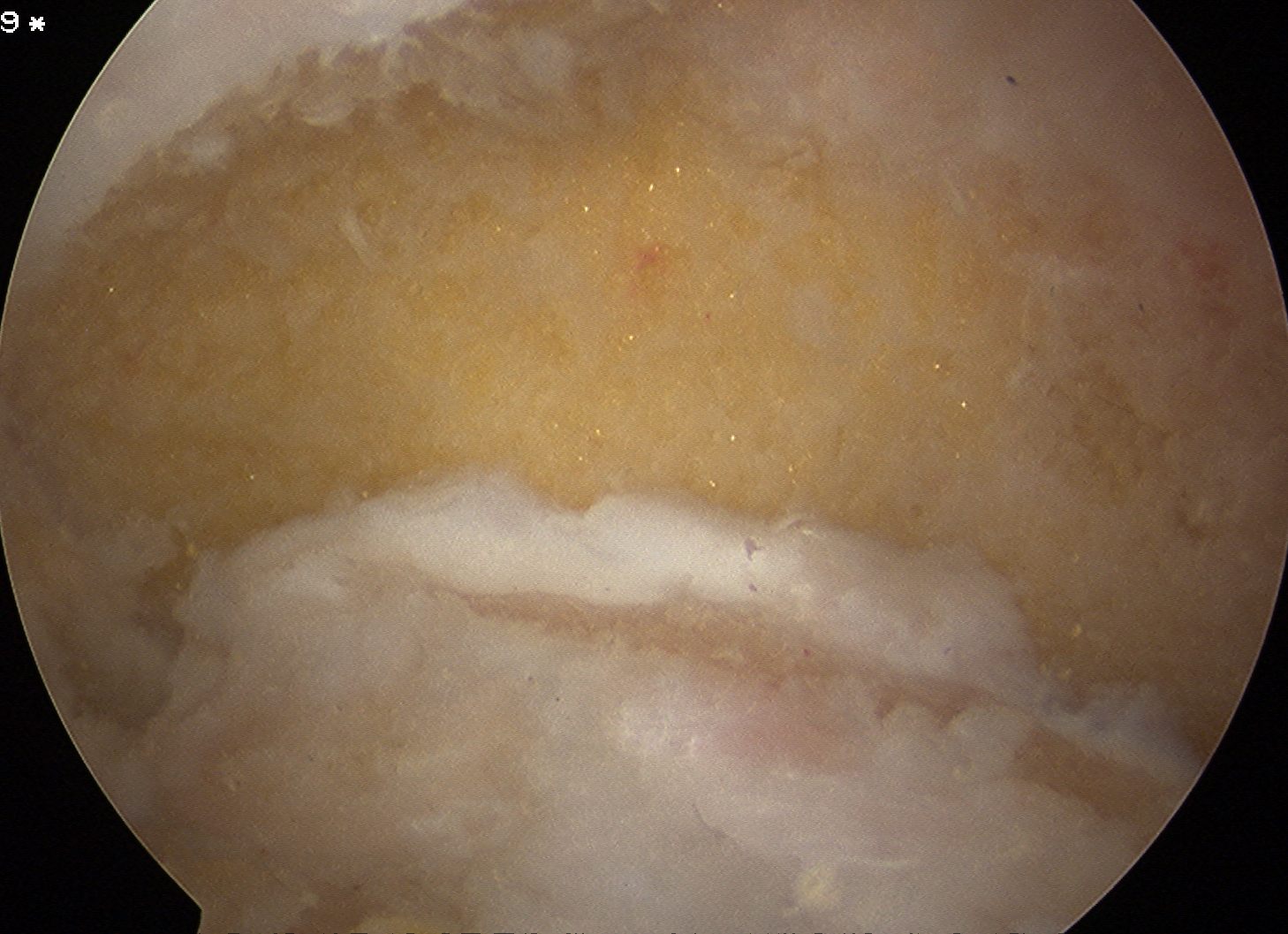
4. Management OCD lesions
5. Synovectomy
- RA, haemophilia
- usually results in marked blood loss
- leave portals open to allow for drainage to prevent haemarthrosis and stiffness
6. Washout sepsis
7. Excision of Radial Head
- useful combined with synovectomy in RA
- can excise head and 2-3mm of neck
- to ensure stability should keep annular ligament
Contra-indications
Abnormal elbow scarring
Extensive HO
Previous ulna nerve transposition
Technique
Equipment
4mm scope
2.7mm wrist scope
Position
A. Patient lateral
- hip supports
- arm over L shaped bolster

B. Patient supine
- anterior portals and arthroscopy with arm on arm board
- posterior portals and arthroscopy with arm bent over patient
Landmarks
Outline surface markings with a pen
- epicondyles, radial head, olecranon
- medial and lateral supracondylar ridge
- draw ulna nerve
PIN landmarks
- anterior to radial head
- posterior to mobile wad
Anterior elbow arthroscopy
Lateral portals
A. Proximal Anterolateral portal
Uses
- intial viewing portal
Technique
- 1-2 cm proximal to lateral epicondyle
- just anterior to lateral intermuscular septum
- onto anterior humerus
- walk down into joint
- insufflate with 20 mls
- incision in skin
- same technique to insert portal
Issues
- radial nerve
- moved further away by insufflation
- most dangerous portal
- do first before swelling obscures anatomy
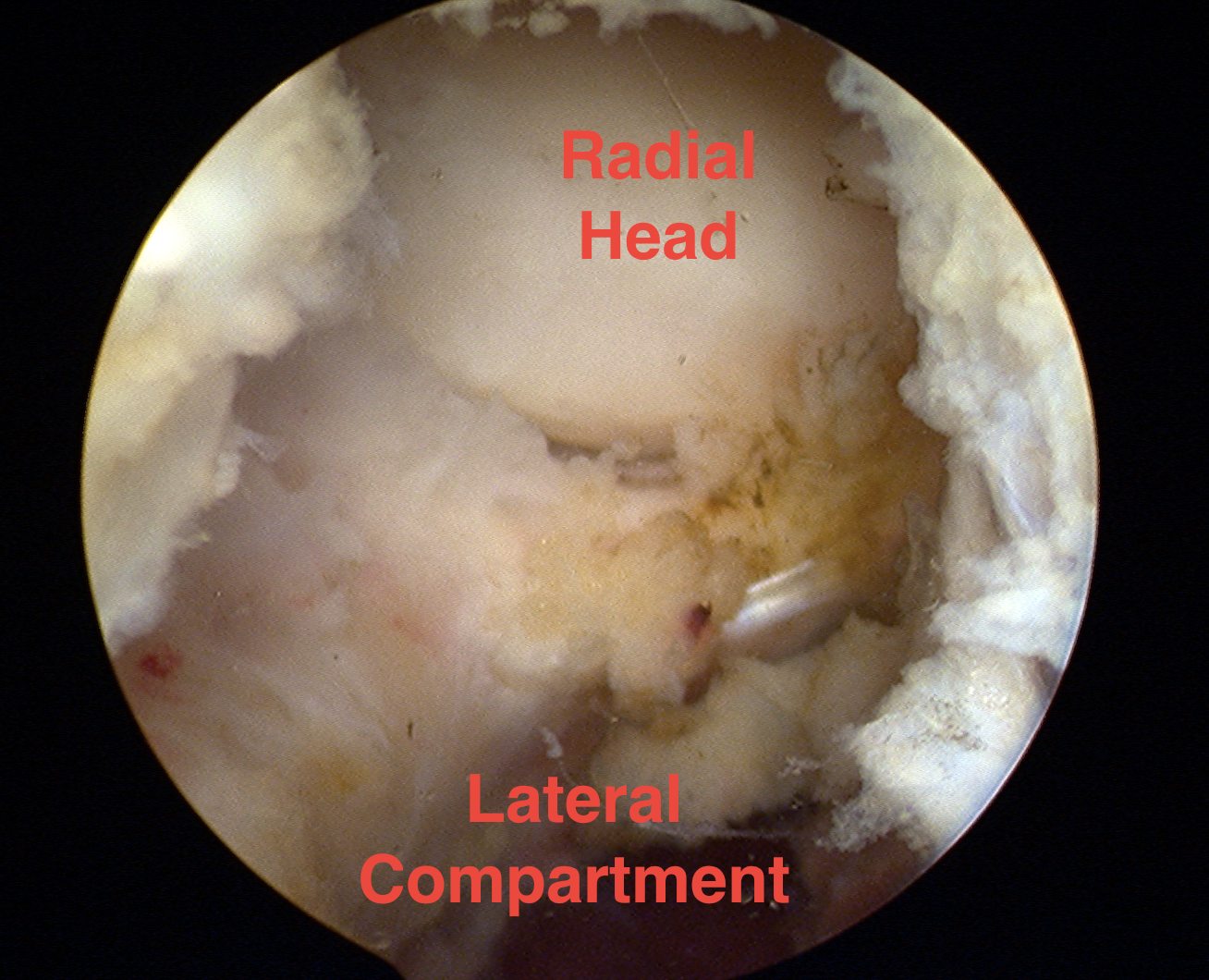
B. Anterolateral Portal
Uses
- working portal
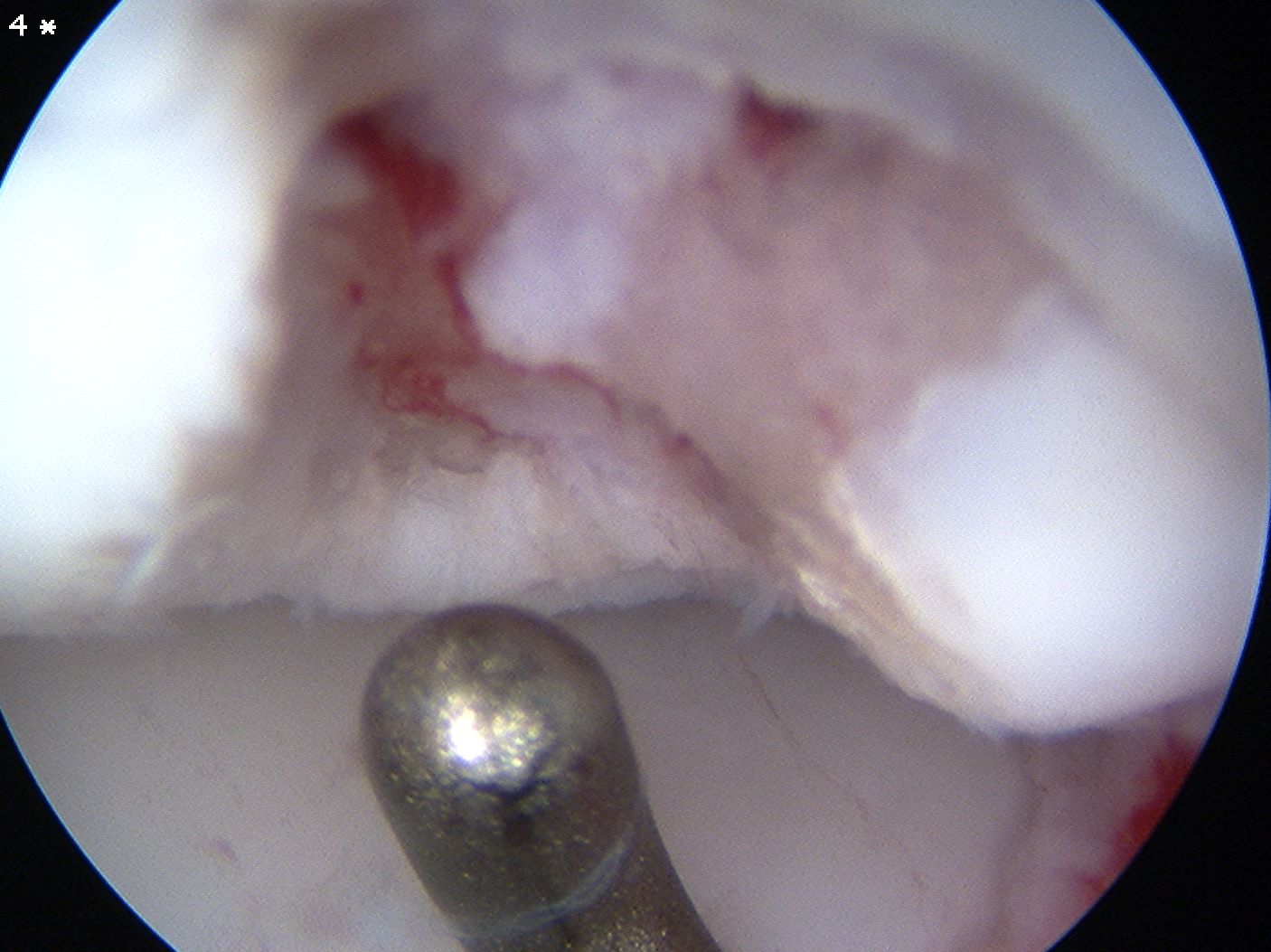
- microfracture capitellar OCD
Technique
- just in front of lateral epicondyle / anterior to radial head
- in sulcus between radial head and capitellum
- PIN most in danger here
- avoid distal / anterior placement
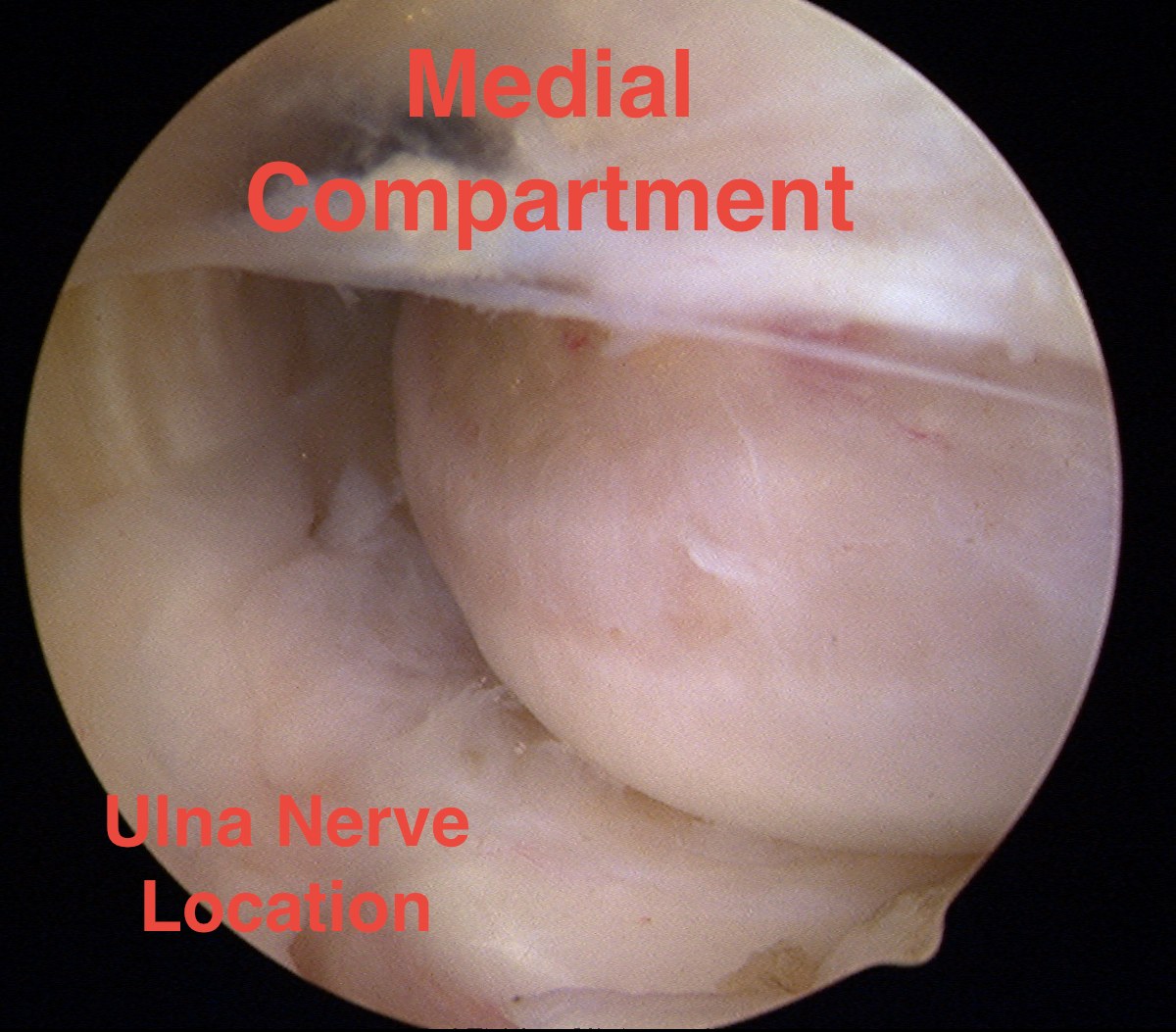
Medial Portals
Proximal Anteromedial Portal
Anatomy
- 2cm proximal to the medial epicondyle
- just anterior to humerus / medial intermuscular septum
- ulna nerve behing medial epicondyle
- median nerve and brachial artery anterior
Technique
- insert needle under vision
- incision in skin
- pass haemostat under vision
Uses
- removal of loose body
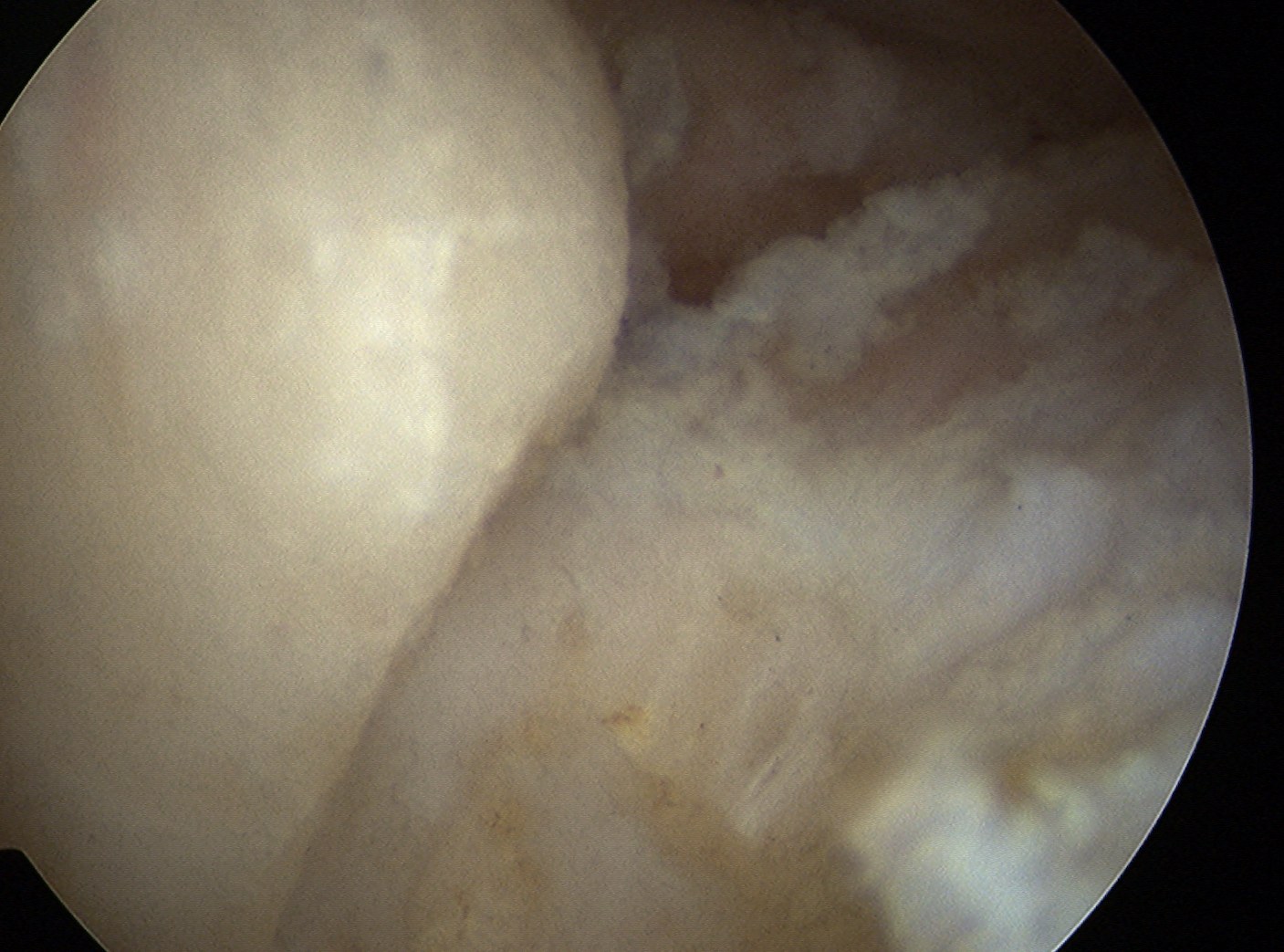
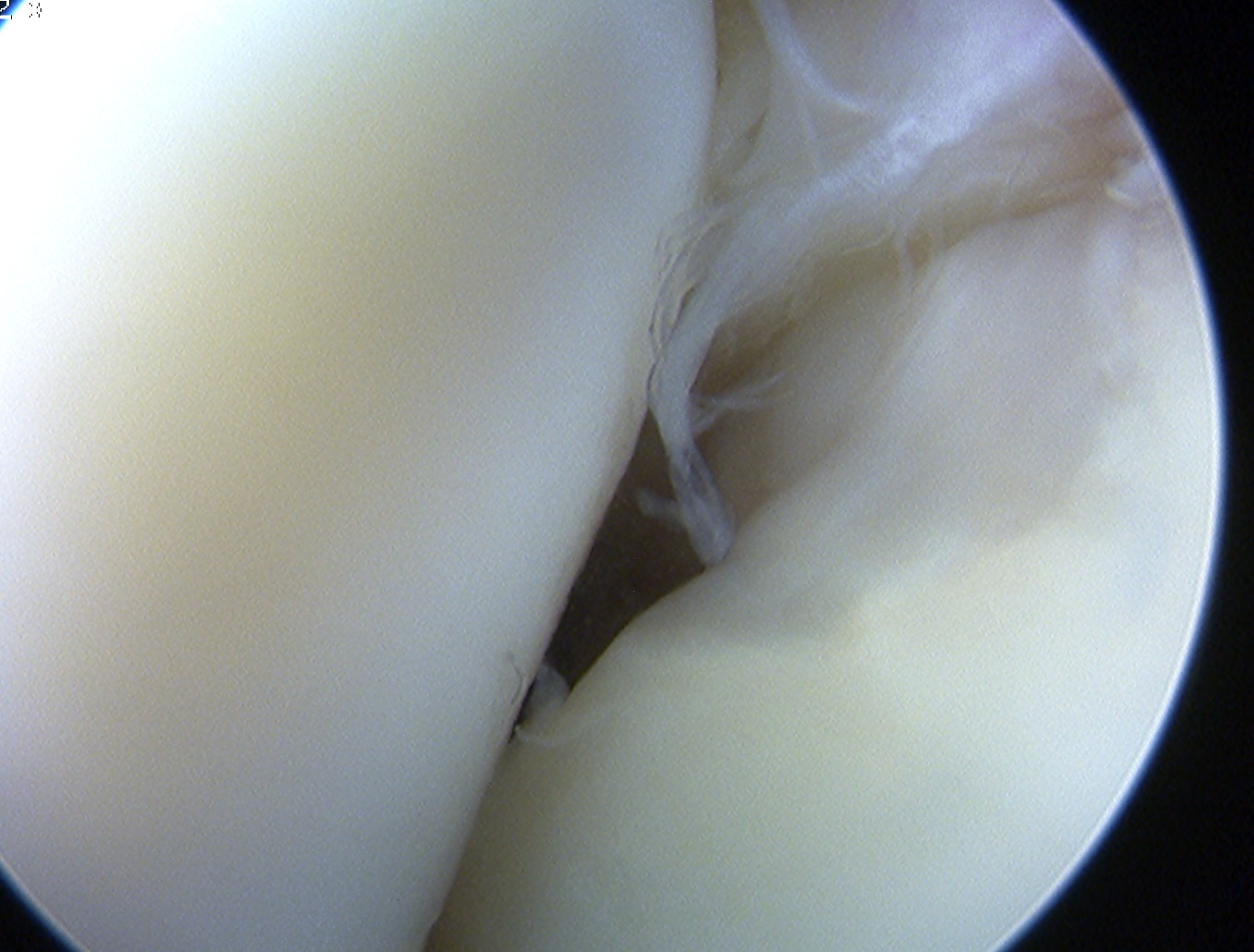
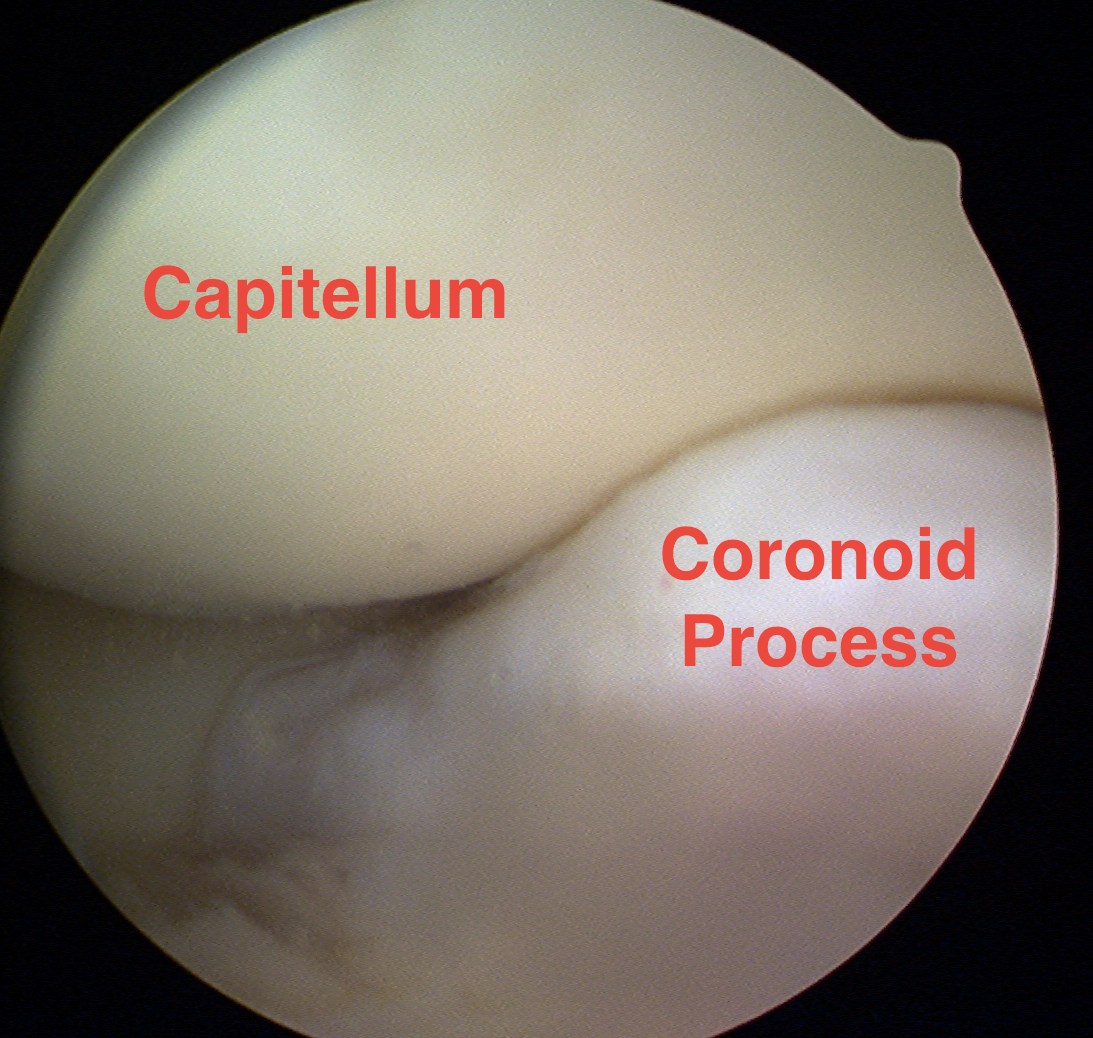
- visualise chondral surfaces ulnohumeral and radiocapitellar
Anteromedial portal
Anatomy
- 2cm anterior and 2cm distal to medial epicondyle
Posterior elbow arthroscopy
Indication
Posterior loose bodies
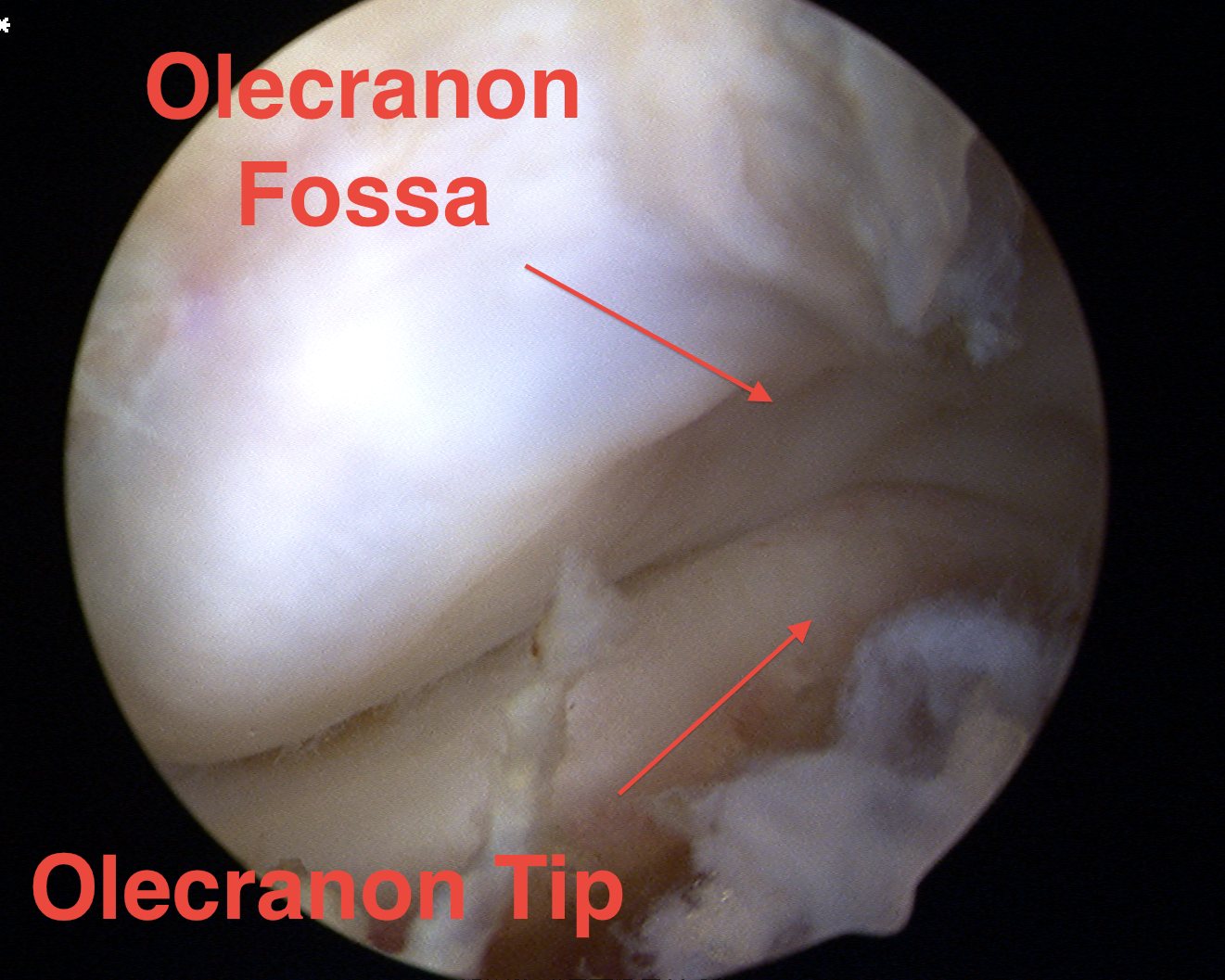
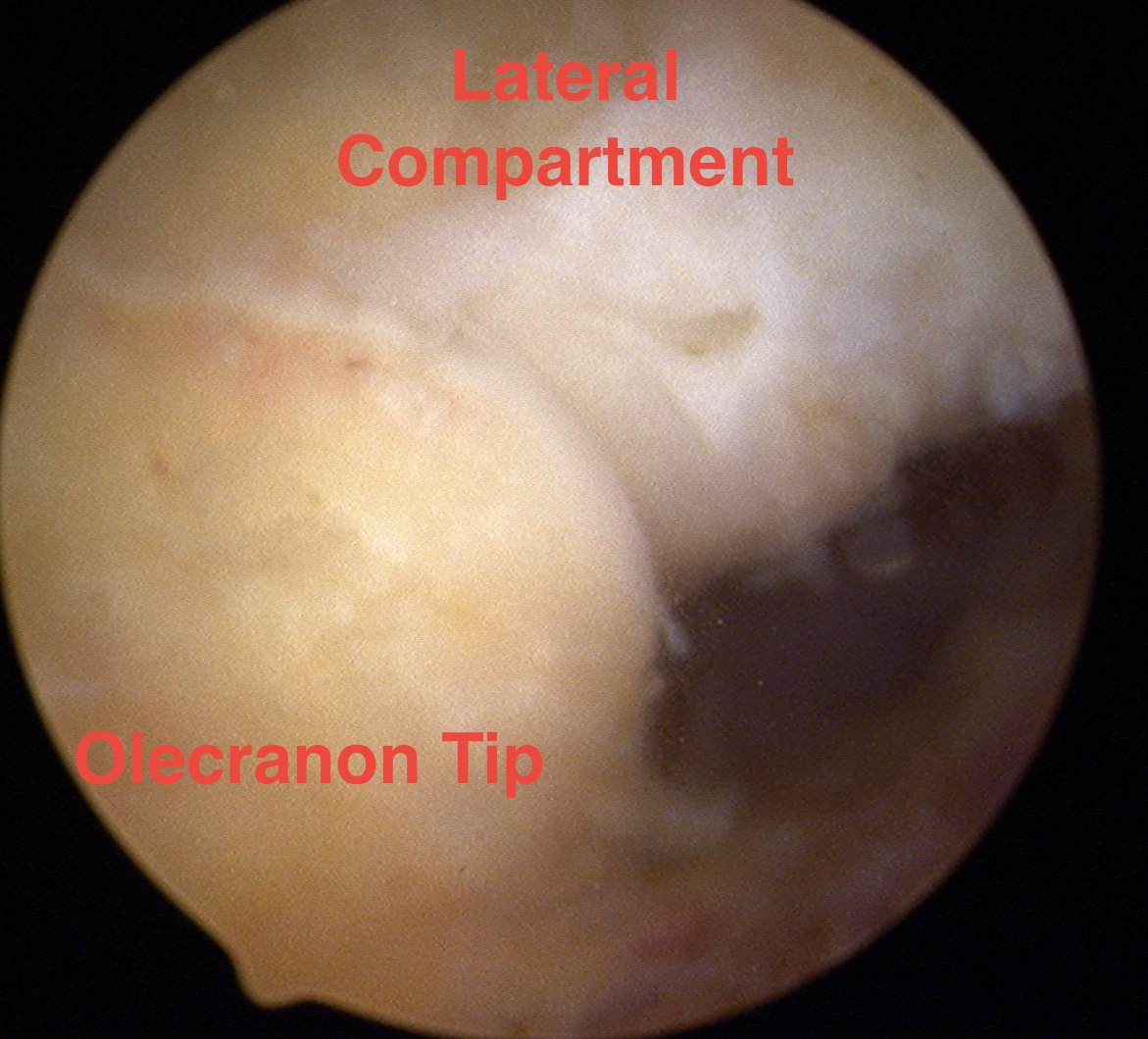
Olecranon tip / fossa impingement
Retrograde capitellum OCD drilling
Danger
- ulnar nerve when debriding medially
Portals
Posterocentral portal
- 3 cm proximal to tip olecranon
- in midline
Posterolateral portals
Technique
- 2 - 3 cm proximal to tip olecranon
- in line lateral edge of triceps
Soft spot portal
Anconeus triangle
- olecranon tip / radial head / lateral epicondyle
- through skin, anconeus, capsule
Danger
- posterior cutaneous nerve
Uses
- retrograde drilling of capitellum
Complications
Nerve injuries
All nerves at risk especially PIN
Always
- no LA
- minimise tourniquet time
- minimise pump pressure to 40
If PIN palsy post op
- need to explore
- usually cut
- very difficult to defend medicolegally
- only do elbow arthroscopy if trained in it and have done cadaver course
Vascular injury
Haemarthrosis
Stiffness
Infection