Bristow
Concept
Non-anatomical bony block
- transfer of coracoid process through subscapularis
- dynamic anteroinferior musculotendinous sling
- provides subscapularis tenodesis
- preventing lower portion from displacing proximally as arm abducted
- when shoulder in vulnerable position abduction and ER

Indications
1. Contact Sportsman
- sportsman who will return to dislocating action and loss of ER not a problem
- football, basketball
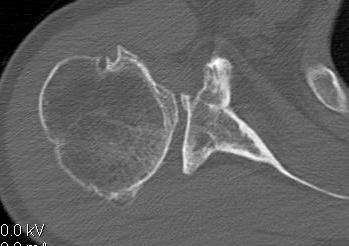
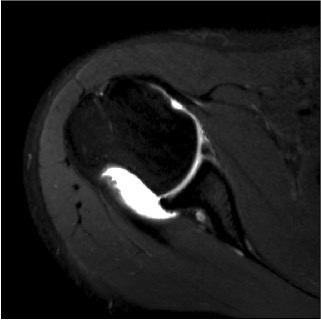
2. Large bony bankart
- > 25 - 30%




3. Large Hill Sachs
- prevent engagement
4. Poor soft tissue
- multiple dislocations
- anterior labrum very poor quality
5. Revision surgery
- i.e. failed arthroscopic or open soft tissue bankart
Problems
1. Loss of ER 12-20°
- problem if throwing athlete
- subscapularis is relatively shortened
2. Screw problems 2-14%
3. Instability 1-20%
- does not address bankart pathology
- difficult to revise with scarring in abnormal positions
4. Injury MCN
Technique
Hovelius
- correct positioning of transferred coracoid process critical to success
- must be near but not over anterior glenoid rim
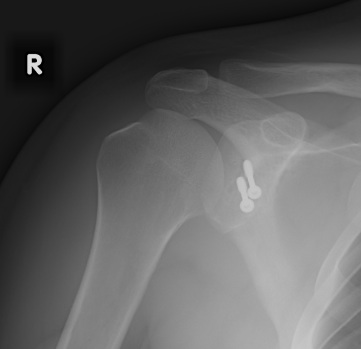
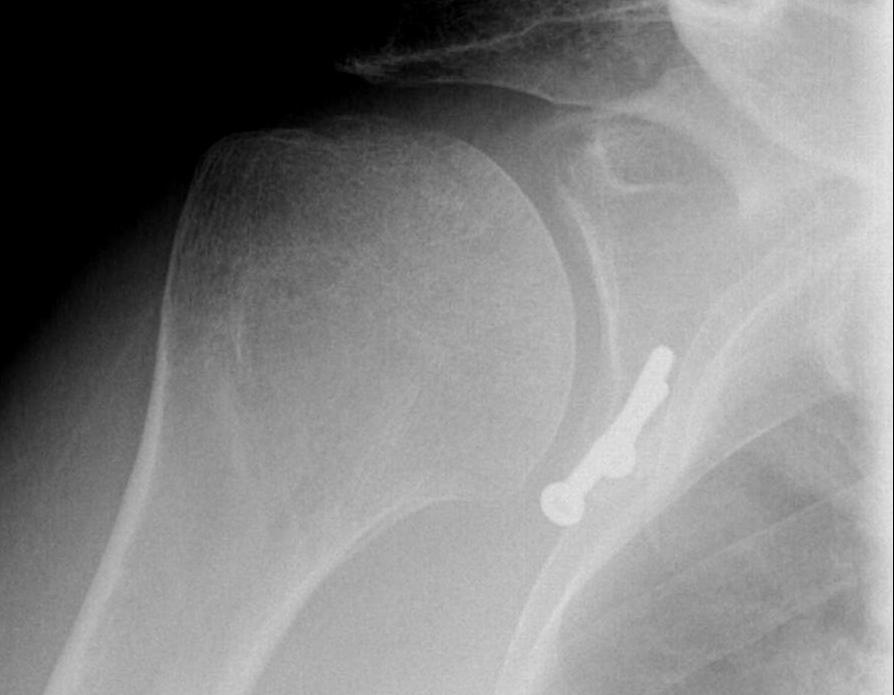
Good results can be correlated with
1. Coracoid process < 5 mm medial to glenoid rim
2. Coracoid positioned inferior to transverse equator of glenoid
3. Bony union develops between coracoid & scapula
4. Fixation screw purchases posterior glenoid cortex
5. Screw does not penetrate articular surface
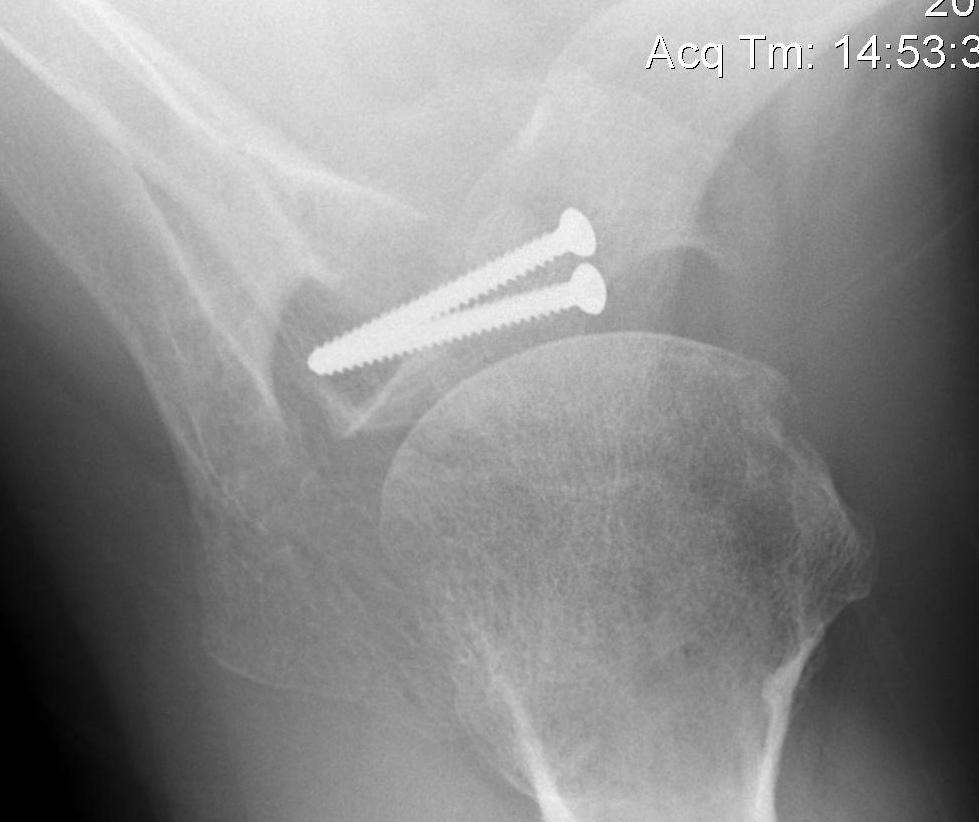
Latarjet
Difference from Bristow
Transfers larger fragment
- allows 2 x screw fixation of coracoid to neck of scapula

Indications
- large > 20-25% bony Bankart
- revision surgery
- contact athlete

Contra-indication
- ? throwing athlete
- can lose considerable ER
Technique
Approach
Deltopectoral approach
- divide clavipectoral fascia at lateral edge of conjoint
Coracoid
Identify coracoid
- use fang retractor on superior surface to identify entire coracoid
- strip Coracoacromial ligament off lateral coracoid
- take pectoralis minor off medially
Divide coracoid
- 3 cm long
- use 90o oscillating blade on microsagittal saw 100
- medial to lateral
Prepare coracoid
- release conjoint for length, identify and protect MCN
- pect minor surface will be placed onto glenoid
- remove cortex with burr
- opposite side clear soft tissue with diathermy
- hold coracoid with Kocher forceps
- make 2 indentations with small burr where 2 x drill holes will be
- stops drill spinning off, ensures drill holes are sufficiently far apart
- 2 x 2.5 mm drill holes, tap, countersink
Deep Approach
SSC
- identify 3 sisters inferiorly
A. Divide muscle transversely at inferior 1/3 of SSC
- at muscle is easier to take off capsule
- also want to be inferior
- do so by inserting scissors and opening blades vertical
- use sponge to separate from capsule
- insert fang superiorly / blunt homan medially for view
B. Take down superior half of SSC
- repair later
Capsule
- feel joint line
- 2 x stay sutures 2 ethibond superiorly and inferiorly
- these must be medially over glenoid
- then divide capsule vertically with knife medial to stay sutures
- want maximum amount of capsule length to repair to anterior glenoid
- this prevents IR contracture
Dissect capsule from SSC
- inferiorly
- medially
- will have a free medial edge to repair to anterior edge glenoid
- may be easier to do this after osteotomy coracoid
- use scissors to dissect capsule superiorly
- beware inferiorly as AXN here
Exposure
- remove retractorr
- insert fukuda to expose humeral head, joint, glenoid
- again use fang / blunt homan superiorly and medially for exposure
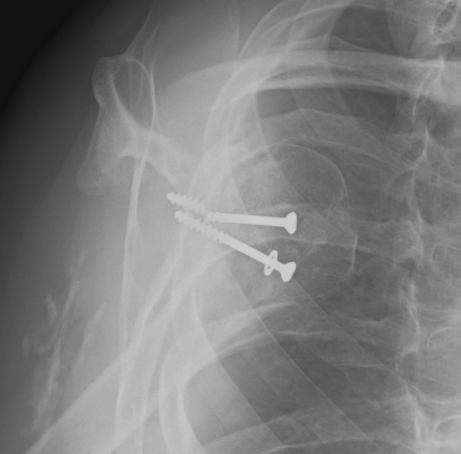
ORIF Bone Block
Bone block
- clear glenoid 3 - 6 o'clock
- need medial area to place bone
- can use burr
- place bone on glenoid using Kockers to hold
- 2 x drill bits, leave first one insitu
- bone must not overhang medially
- bicortical, tap, typically 30 - 40 mm partially threaded cancellous

Capsule repair
Remove Fucuda
- find capsue with stay sutures
- insert 2 x 3 mm absorbable anchors 3 and 5 o'clock
- pass in mattress formation through capsule
- can use Depuy Mitek Suture grasper
- pass this through capsule lateral to medial, grasp suture
- tie capsule down, ensure knot goes down past bone block to glenoid
Results
Burkhart et al Arthroscopy 2007
- 102 procedures for patients with the inverted pear glenoid +/- engaging Hill Sachs
- 4.7% recurrence rate
- 5o loss or ER
Boileau et al Arthroscopy 2010
- arthroscopic Latarjet
- 6/47 had to be converted to open
- no recurrence of instability at 16 months
- 1 bony block fracture and 7 migrations
- potentially dangerous and difficult procedure
Complications
Failure of fixation
Non union of coracoid
- need to carefully prepare both surfaces
- good compression
Suprascapular nerve injury
- screws too long, or too superior
OA
- bone block too medial
Dislocation
- too high, can dislocate under bone block
- too low, can dislocate over bone block