Vessels at risk
| Extra-pelvic blood vessels | Intrapelvic vessels |
|---|---|
|
Femoral Artery MCFA LCFA Profunda Femoris Obturator artery |
External iliac artery and vein Obturator artery Superior and inferior gluteal |
External Iliac Vessels
Anatomy
Anterior division of common iliacs / L5-S1
- runs down medial border of psoas
- psoas separates external iliacs & intrapelvic surface of anterior column
Injury
Anterosuperior screws
- significant intrapelvic bleeding may occur before diagnosis
- vein more at risk than artery
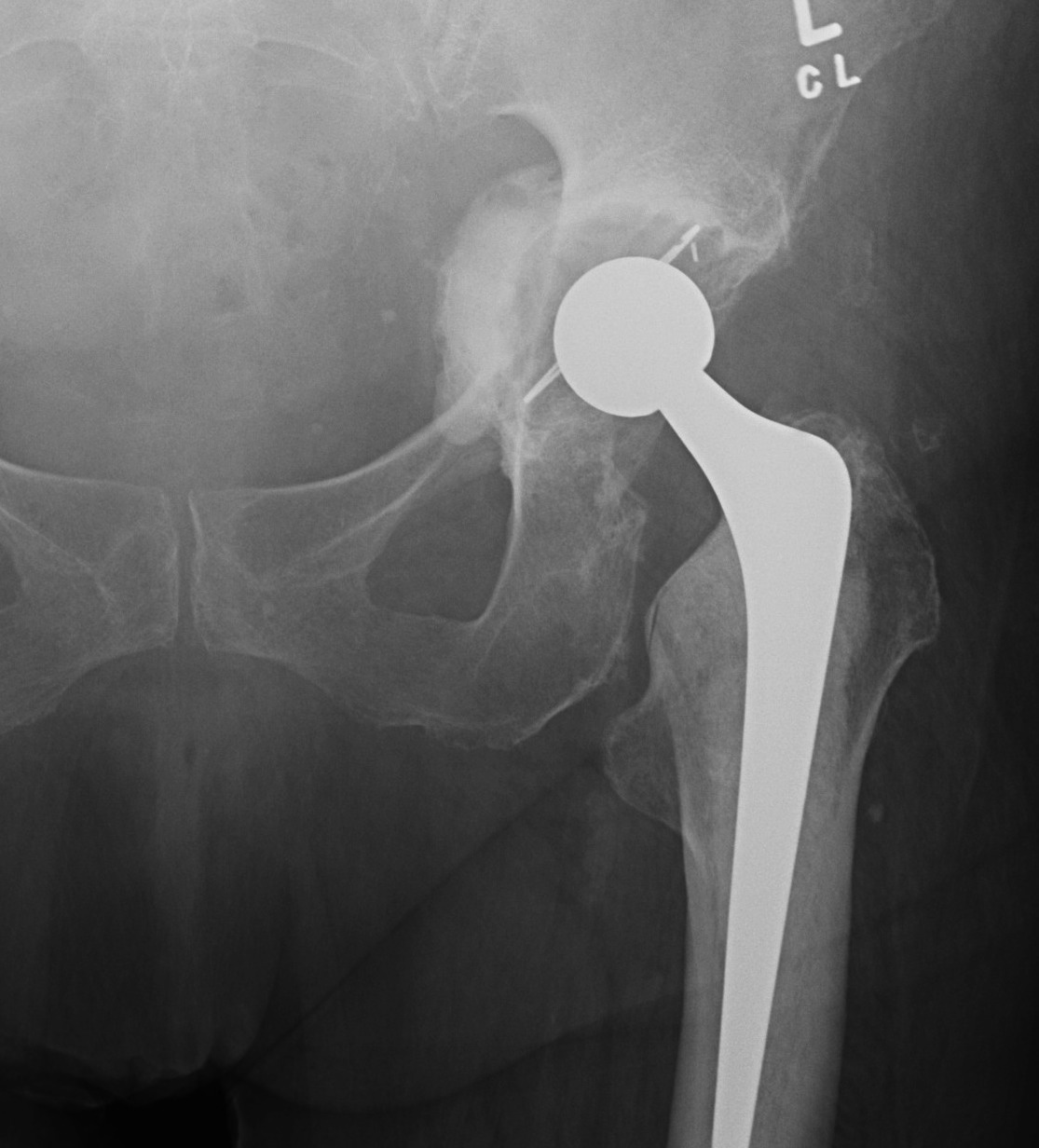
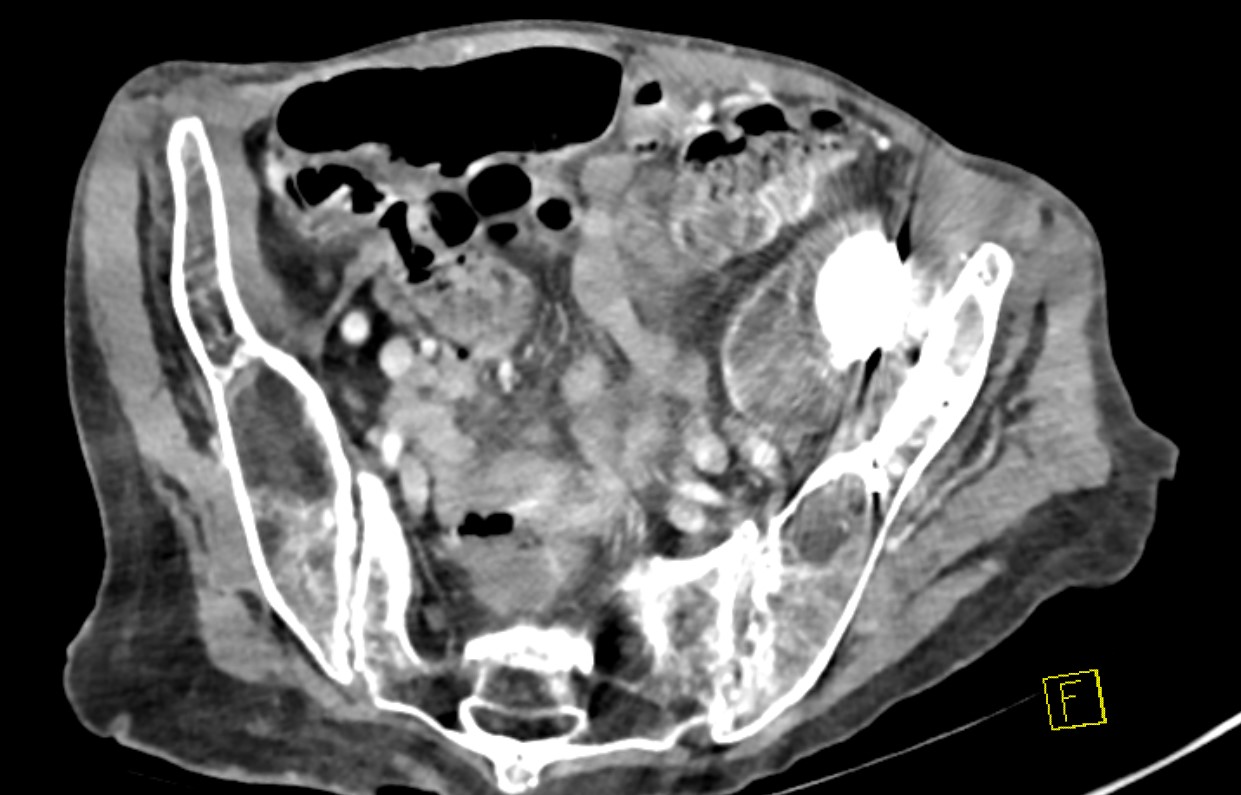
Intra-pelvic cement / components
- danger with removal / revision
- CT angiogram pre-operatively
- may require separate intrapelvic exposure
- alert general surgeons / vascular surgeons

Femoral blood vessels
Most commonly injured
Anatomy
Common femoral artery
- continuation of EIA as passes under inguinal ligament
- passes anterior to hip capsule
- separated from it by psoas
Injury
Anterior retractors / dissection
Anterior quadrant screws and drills
Obturator blood vessels
Anatomy
Traverse lateral wall
- separated from quadrilateral plate by obturator internus
- lie at superolater aspect of obturator foramen
- exit pelvis via obturator canal
Injury
Screws in AI quadrant
Retractor under transverse acetabular ligament
Management
Bleeding at inferior transverse ligament
- can be very difficult to ligate
- pack with swab
- hold swab with inferior retractor
- finish acetabulum
- will usually be controlled
+/- embolization
Superor gluteal blood vessels
Anatomy
Branch posterior division internal iliac artery
- close to posterior column
- exits greater sciatic notch above piriformis
Injury
Screw near sciatic notch
Inferior Gluteal & Internal Pudendal vessels
Anatomy
Branch anterior division internal iliac
- exit pelvis between piriformis & coccygeus
- close to posterior column near ischial spine
- internal pudendal artery re-enters pelvis through lesser notch
- inferior gluteal artery passes under piriformis
Injury
Very long screws through posterior column
Management on table severe bleeding
Anaethetist
- IV fluids
- Bloods - coags, CBC, platelets, cross match
- transfuse blood +/- platelets
- organise cell saver
Control bleeding
- call vascular surgeon
- pack & wait
Vascular surgeon
- Ilioinguinal approach - clamp IIA, vessiloop IIV
- Retro-peritoneal approach / Rutherford-Morrison incision
Post-operatively
- angiography
- transcatheter embolisation