1. MPFL reconstruction
Indication
- patient with history initial traumatic dislocation
- also indicated in patient with laxity to act as a check rein
Grafts
1. Y Graft
- double ST autograft into Y
2. Single limb free semitendinosus autograft
- limb to patella via endobutton

Schottle's Point
Schottle AJSM 2007
- cadaveric study
- 1 mm anterior posterior cortex
- 2 mm distal to MFC origin
- above blumensaats

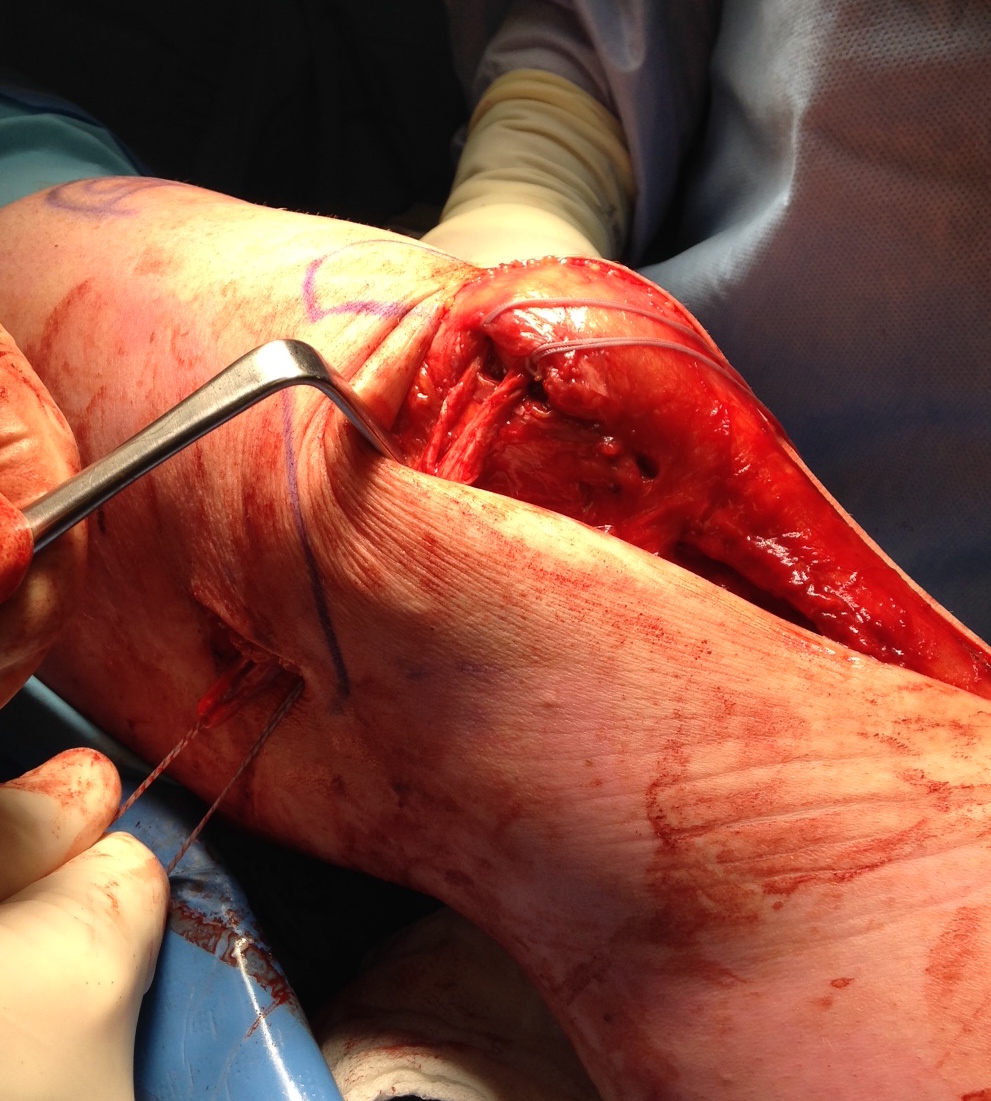
Technique
A. Patella fixation
- incision along medial patella
- 2 drill holes in patella
- attach ends of graft, pass into patella, secure with anchor of choice
- pass graft superficial to capsule
B. Femoral fixaiton
- best to use II to find point
- stem between medial epicondyle and adductor tubercle
- Schottle's Point
- drill wire across femur, drill hole for fixation screw
- pass doubled graft into tunnel
- set at 30o flexion
- ensure doesn't dislocation laterallly
- don't overtighten
- secure with screw
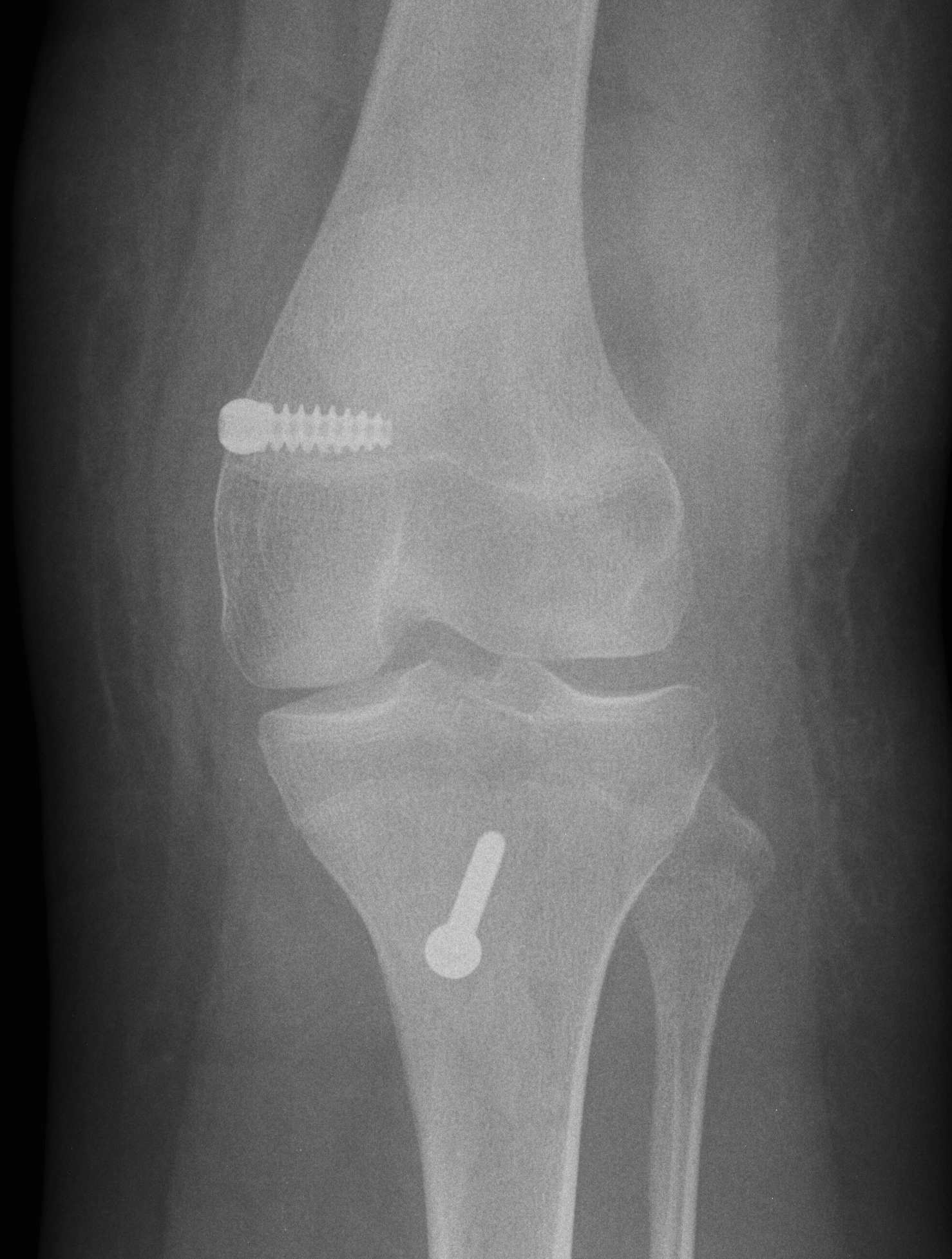
Xrays 1
Tunnel too anterior / tight in flexion
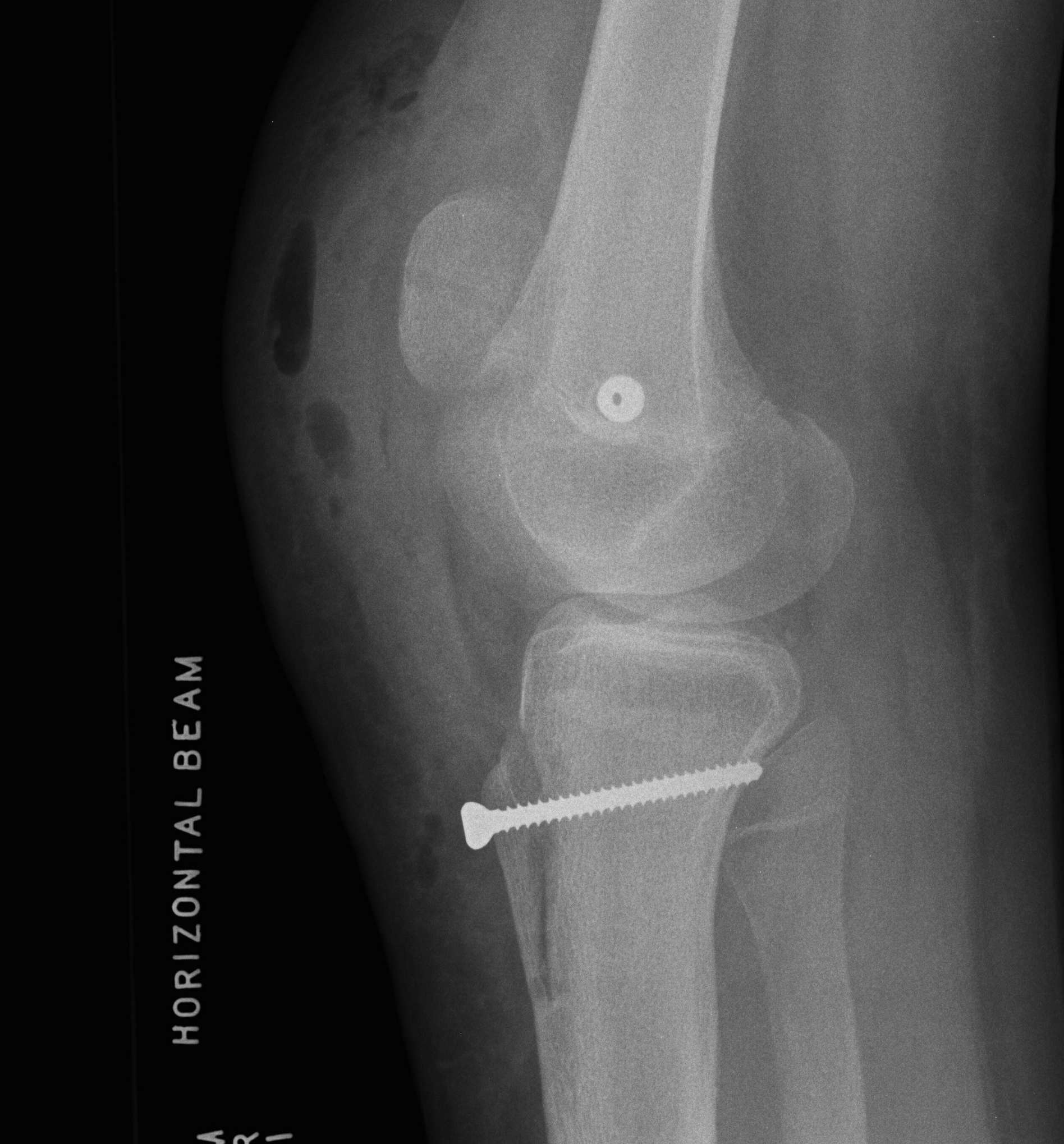
Xray 2
Finding Schottles Point

Results
Nomura et al J Arthroscopy 2006
- recurrent dislocation, no malalignment
- 83% G/E results
- no redislocation at 2 year follow up
Howells JBJB Br 2012
- 211 procedures in 193 knees
- all TTTG < 18
- most moderate trochlea dysplasia
- no redislocations at 16 months
Shah et al AJSM 2012
- Systematic review MPFL
- 26% complication rate
- 4/629 (0.6%) fractures
- 26/629 (4%) stiffness
- 23/629 (3.7%) failure rate