Disectomy Technique for Posterolateral L4/5 disc
Anatomy
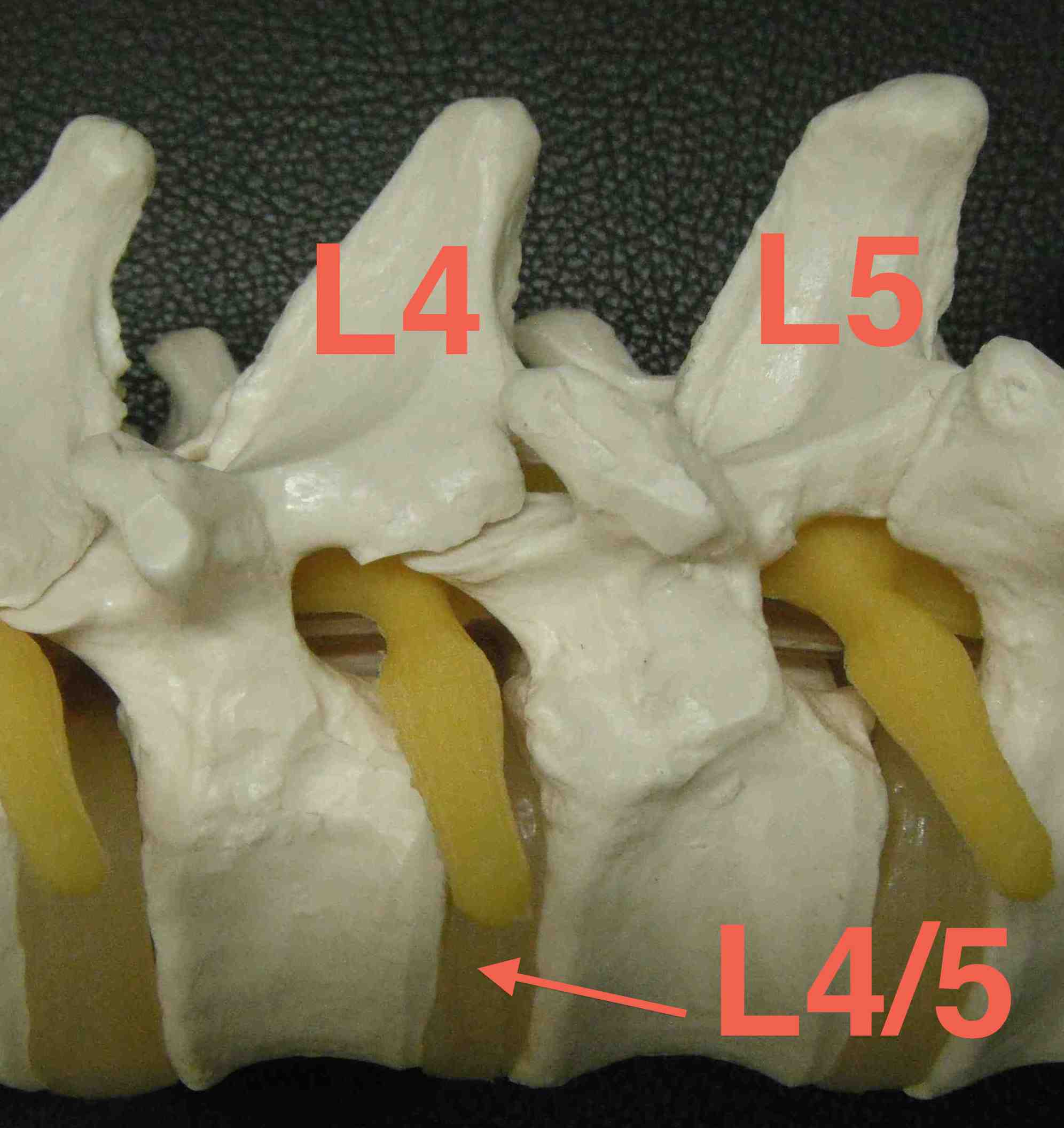
L4/5 disc at level of facet joints
Interlaminar space is below disc
- have to take inferior aspect of superior lamina
Pedicle and transverse process at same level
Disc usually on one side
- hemilaminotomy
- no need to remove spinous process
- this preserves stability
Position
4 poster support
- abdomen free (decrease venous drainage) / Jackson Table
- knees below hips
- pillows under legs and feet
- pressure care knees
- arms forward on supports
- back level & slightly head down
- protect eyes / CPN at knees / ulna nerve at elbows
Pre-Operative antibiotics
Often dressing + betadine in natal cleft
Levels
Careful correlation of clinical and MRI
- level of disc
- side of disc
Iliac Crests L4/5
- mark
- prep with antimicrobial solution
- insert 18G needle into L4/5 interspinous space
- obtain cross table xray to confirm level
- this centres incision
Incision
Square drape
LA with adrenalin
Incise skin L4 spinous process to S1 spinous process
Superficial Dissection
Divide thoracolumbar fascia
- in midline down to spinous processes
- subperiosteal dissection down side of spinous process
- with cobb / diathermy
- preserve suprasinous ligament
Subperiosteal dissection to lamina on lesion side
- expose but don't disturb facet joint capsule
- self retractor inserted
- don't go between transverse processes
Lamina spreader between spinous processes
- under supraspinous ligament
- opens up interlaminar space
Recheck level at L4/5 interspinous

5 ways to identify L5/S1
Sacrum
- hollow sound
- non mobile
- midline crest with no ligamentum flavum / interlaminar space
- anterior slope L5 lamina
- large L5 S1 interlaminar space

Deep Dissection
Expose Ligament Flavum
- attaches on top of inferior lamina to superior lamina
- find midline raphae
- incise flavum with scalpel over inferior laminae
- create flap of flavum
- use Watson Cheyne Dissector to gently dissect off dural adhesions
- remove flavum laterally
- 1, 2 or 3 mm 40° Kerrison Rongeur
- see fat overlying blue dura
Remove inferior aspect of superior lamina
- will take up to L4/5 disc
- resect medial two thirds of superior facet / lower one third inferior facet


Exiting L4 nerve root
- above L5 pedicle
L5 nerve root
- below L5 pedicle
- remove inferior lamina and pars
Discectomy
Retract dura gently
- dural retactor
- remove sequestered disc with pituitary rongeur
- cruciate incision in PLL to remove protruding / extruding disc
L5 nerve root
- exit under pedicle L5 inferiorly
- medial facetectomy
- follow root out laterally around pedicle
- ensure free passage through foramina
- should be able to pass Watson Cheyne easily
L4 nerve root
- L3/4 interlaminar space
- remove inferior lamina and pars
- will pass under pedicle of L4 inferiorly
- medial facetectomy of L3/4 facet joint
- access L4 pass under pedicle of L4 superiorly
Wiltse Approach to Extra-Foraminal Disc
Incision
Paramedian incision
- 2 fingerbreadths / 5cm lateral to midline
Superficial Dissection
Muscles split to intertransverse ligament
- between Longissimus & Multifidus
- always a bleeder on the way down
- clear transverse processes
- preserve posterior ramus by hooking finger around & then follow ramus to nerve
Deep Dissection
Removed intertransverse ligaments and fascia between TP
- nerve root anterior to fascia and just below TP
- runs at a 45o angle
- follow nerve medially and identify disc
- retract nerve laterally & remove disk
- may have to incise annulus to remove bulge
- if intra-foraminal element, remove lateral facet
Post operatively
Symptoms should be immediately relieved
Analgesia
Watch retention
No anticoagulation
Mobilize ASAP
No heavy lifting 6/52