Epidemiology
0.05% incidence
- rare due to stabilising effect of rib cage
- even more rare to have symptoms
Reasoning
1. Discs are narrower
2. Foramina larger
3. Thoracic spine
- facet joints orientated for rotation
- lumbar spine for flexion extension
- flexion is typically the motion which ruptures annulus
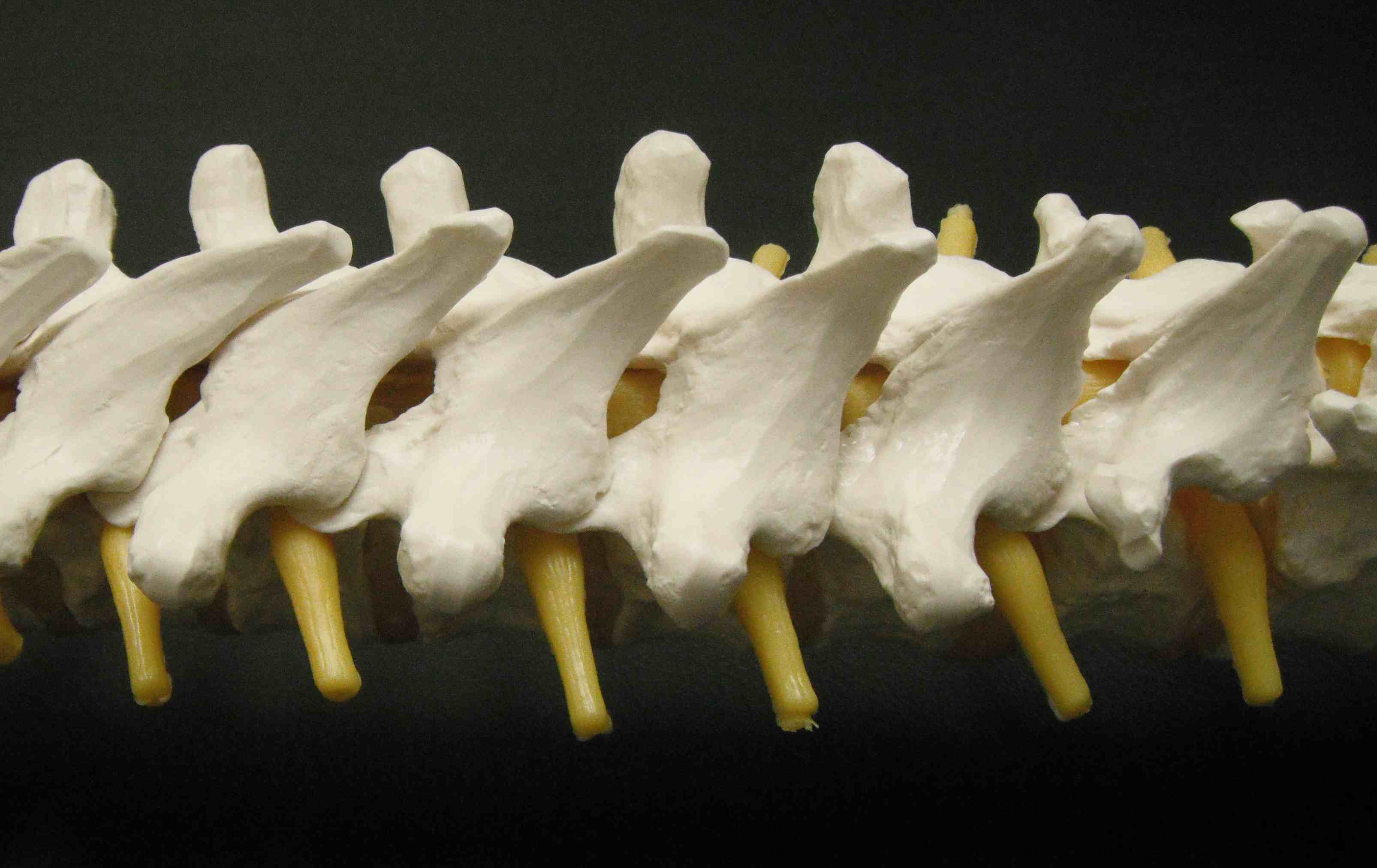
Anatomy
Increase in size from T1 to T12
- small pedicles
- long spinous processes
- relatively large intervertebral foramina
- facets nearly vertical
- TP come off the pedicle
- costal articulation TP and vertebral body
Clinical
Present with intercostal radiculopathy or myelopathy
Xray
Disc space narrowing / degenerative changes
> 50% thoracic discs associated with calcified disc material in canal
- probably indicates chronicity


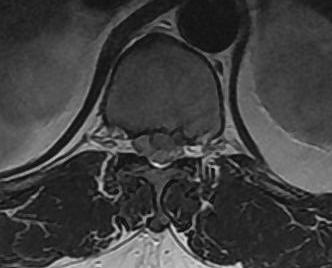
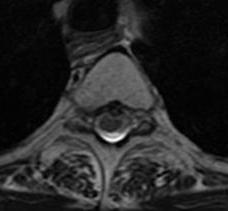
MRI
Very sensitive
- 40% incidence asymptomatic thoracic disc protrusion


Management
Non Operative
Indication
- single level disease
- no myelopathy
- operation rarely indicated
- usually settles with physiotherapy / analgesia
Operative
Indications
- myelopathy
- unrelieved radiculopathy
Options
Posterior approach / discectomy via laminectomy
- contraindicated
- spinal cord does not tolerate retraction
Anterior Approach
- costotransversectomy
- corpectomy (2 level disc)
A. Thoracotomy and Costotransversectomy
Definition
- resection of rib + transverse process
Indication
- single level disc resection
- unilateral disc
Technique
- posterior approach
- remove of rib and transverse process
- ipsilateral pedicle removal
- removal disc protrusion
B. Thoracotomy and Corpectomy
Indication
- 2 level disc protrusion
Technique
Thoractomy Approach
- loin incision
- removal of rib 2 levels above
- through bed of rib
- extrapleural approach
- from left to avoid IVC
Tie off segmental artery on one side
- disc convex, body concave
- allows access to disc protrusion
- discectomy + / - corpectomy as required for exposure / 2 level disc
- anterior +/- posterior stabilisation if corpectomy
- if simply remove disc may not need stabilisation especially in elderly
- will autofuse

Complications
Cord injury
Cord infarct
- ligation segmental artery
- exceedingly rare with unilateral approach
- much higher risk with bilateral approaches
- CTA to look for artery adamkiewicz
Intercostal neuritis
- not uncommon
- treat with repeated intercostal nerve blocks
Bleeding
- usually from segmental artery
- patient presents difficulty breathing / hemothorax
- may have high output from drain
- > 200mls / hour clamp drain and urgent return to OT with vascular surgeon