Incidence
Lateral : Medial 9:1
Epidemiology
4th & 5th decades
- M = F
- 75% dominant arm
50% of regular tennis players
- especially > 2 hrs / week
Aetiology
Insertion pathology / Enthesopathy
Over-extension of the elbow with supination / pronation
Anatomy
Lateral epicondyle
- anconeus from posterior face
- ECRB and EDC from anterior face (CEO)
- ECRL and BR from lateral supracondylar ridge
Differentiate ECRB from ECRL
- ECRB tendinous insertion onto lateral epicondyle
- ECRL still muscular at this point (arises more proximally)
LCL
- apex of lateral epicondyle
PIN
- radial nerve between brachialis and BR
- divides at level of radial head
- enters supinator at this level (radial tunnel)
DDx
1. OCD capitellum / radial head
2. Radial tunnel / supinator / PIN syndrome
3. PLRI
4. OA, RA
5. Referred Pain / C6-7 radiculopathy
6. Enthesopathy
7. Annular ligament tears
Risk factors
Tennis
- poor technique
- poor grip
- hard court surfaces
- strings too taut
Occupational
- plumbers
- painters
Pathophysiology
Starts as micro-tear in ECRB
Get high grade partial tear
Histology
Angiofibrotic hyperplasia
- marked fibroblast proliferation
- extensive vascular hyperplasia
- disorganised collagen production
- may go on to dystrophic calcification
Disruption of parallel orientation of collagen fibres
- invasion of fibroblasts and vascular granulation type tissue
- without an acute or chronic inflammatory component
History
History of overuse
Pain lateral elbow
Backhand in tennis main problem
Examination
Localised Swelling
ROM
- few degrees loss of extension = CEO
- >15-20° loss is intra-articular pathology
Tender ECRB
- 5 mm distal and anterior to CEO
Test
- pain with resisted wrist dorsiflexion with elbow extended
Examine for Stability - PLRI
Examine Supination / Pronation - radiocapitellar OA
Examine C spine
DDx
Radial Tunnel Syndrome
- tenderness 3-4 cm distal to lateral epicondyle
- pain with resisted thumb / IF and supination
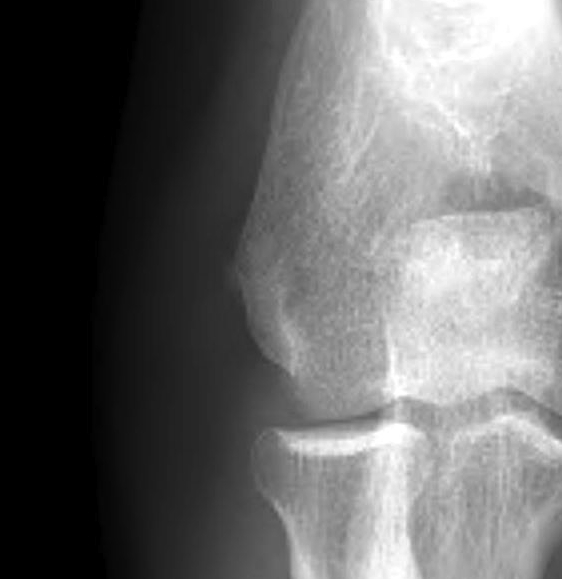
Xray
Usually normal
25% soft tissue calcification

NCS
Normal
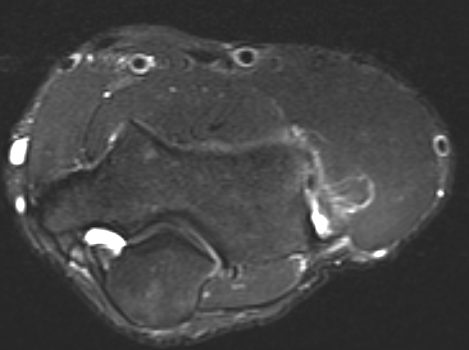
MRI
Will demonstrate tears and oedema on T2

High grade partial tear
Management
Non Operative
Timing
6-9 months
- successful ~ 75- 85%
Rest Phase
Complete rest lasting for 3-6/52
- avoid precipitating factors
NSAIDs
- oral or topical
Brace
- wrist in extension
- cock up wrist splint
Forearm tennis band
- limit muscle expansion
- may create new force direction
HCLA injection
- find patient's maximum tenderness deep to fascia
- repeat 2-3 times over 6-12 months
- peri not intra-tendinous
- must then rest the tendon for it to work long term
- risks of local skin depigmentation and CEO rupture
Conditioning Phase
Once pain settled
- Extensor origin stretching
- Wrist extension exercises (1lb increments)
- eccentric muscle training
- ART (active release technique)
- Activity modification / change racquet and stroke
Tyler et al J Should Elbow Surg 2010
- RCT using eccentric muscle training
- significant improvement in outcome
Adjuctive Therapy
1. Shock wave lithotripsy
Meta-analysis of RCT
- minimal effect comparted with placebo
2. Autologous Blood / PRP Injections
Peerbooms et al Am J Sports Med 2010
- RCT autologous blood v corticosteroid
- superior outomes with plasma cell injections at one year
3. Botox Injections
Improvements compared with placebo
Inferior to corticosterioid
Operative Management
Indication
Failure of good non-operative management
- > 6 - 12/12
Options
- open debridement
- percutaneous tenotomy
- arthroscopic
- radiofrequency microtenotomy
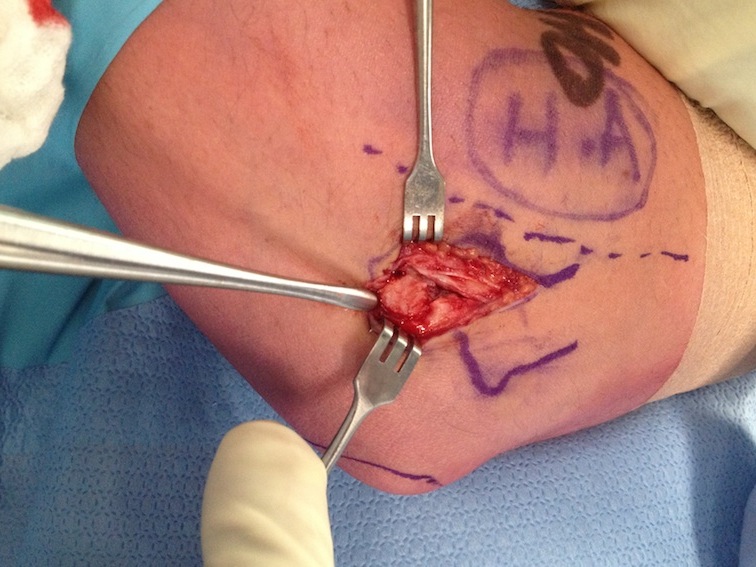
Open debridement
3 cm incision
- centred on CEO
- ECRB is deep and posterior to ECRL
- ECRL muscular at this point
Surgical dissection
- Detach ECRB
- Debride degenerative tissue
- Decorticate underlying CEO
- +/- reattach ECRB



Modifications
- Z lengthen
- denervate sensory nerves to epicondyle
- combine with decompression PIN
- cover with anconeus flap in chronic or recurrent cases
Post-op
- splint 10 days
- gentle ROM to 6/52
- then strengthening exercises
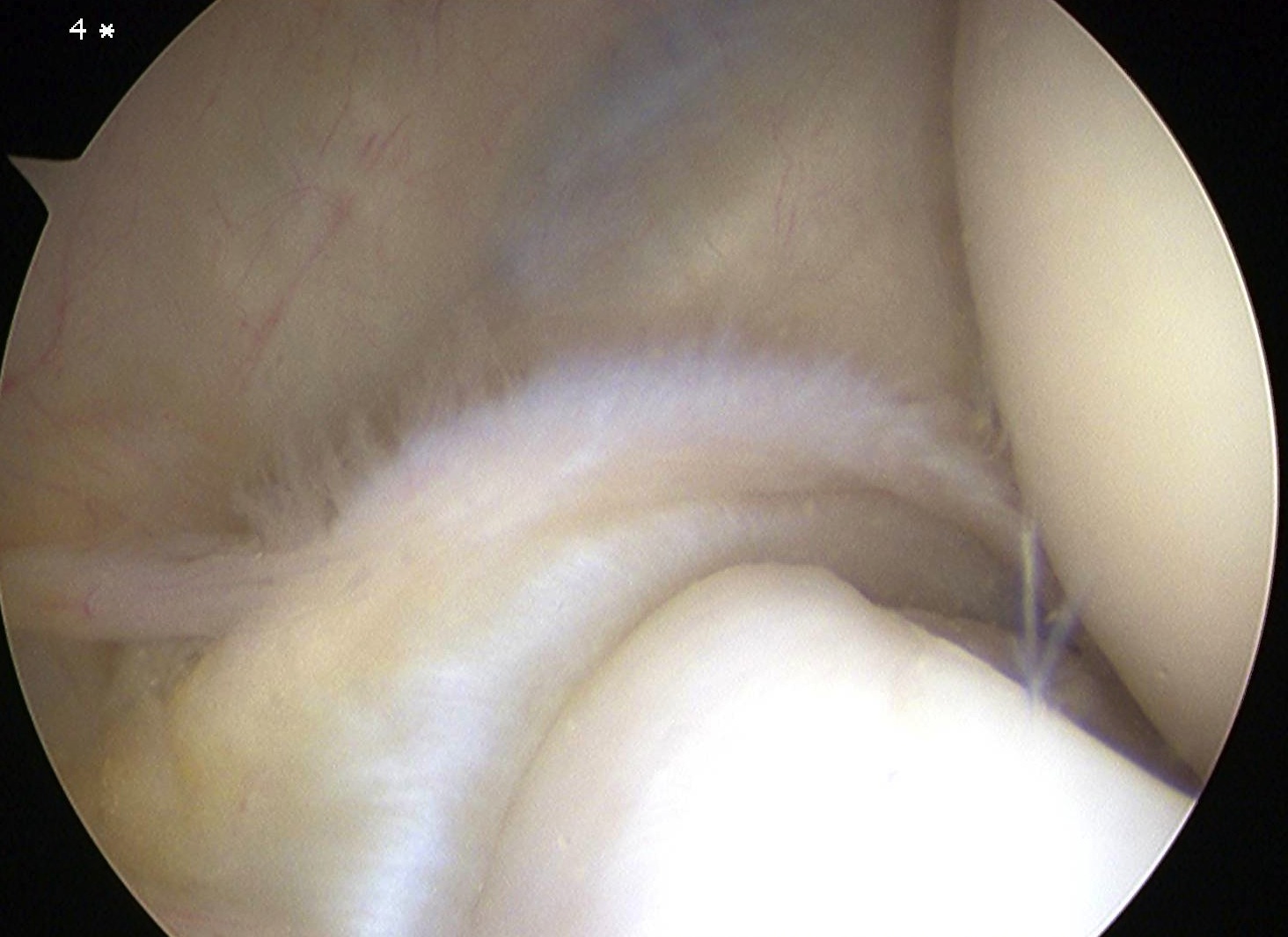
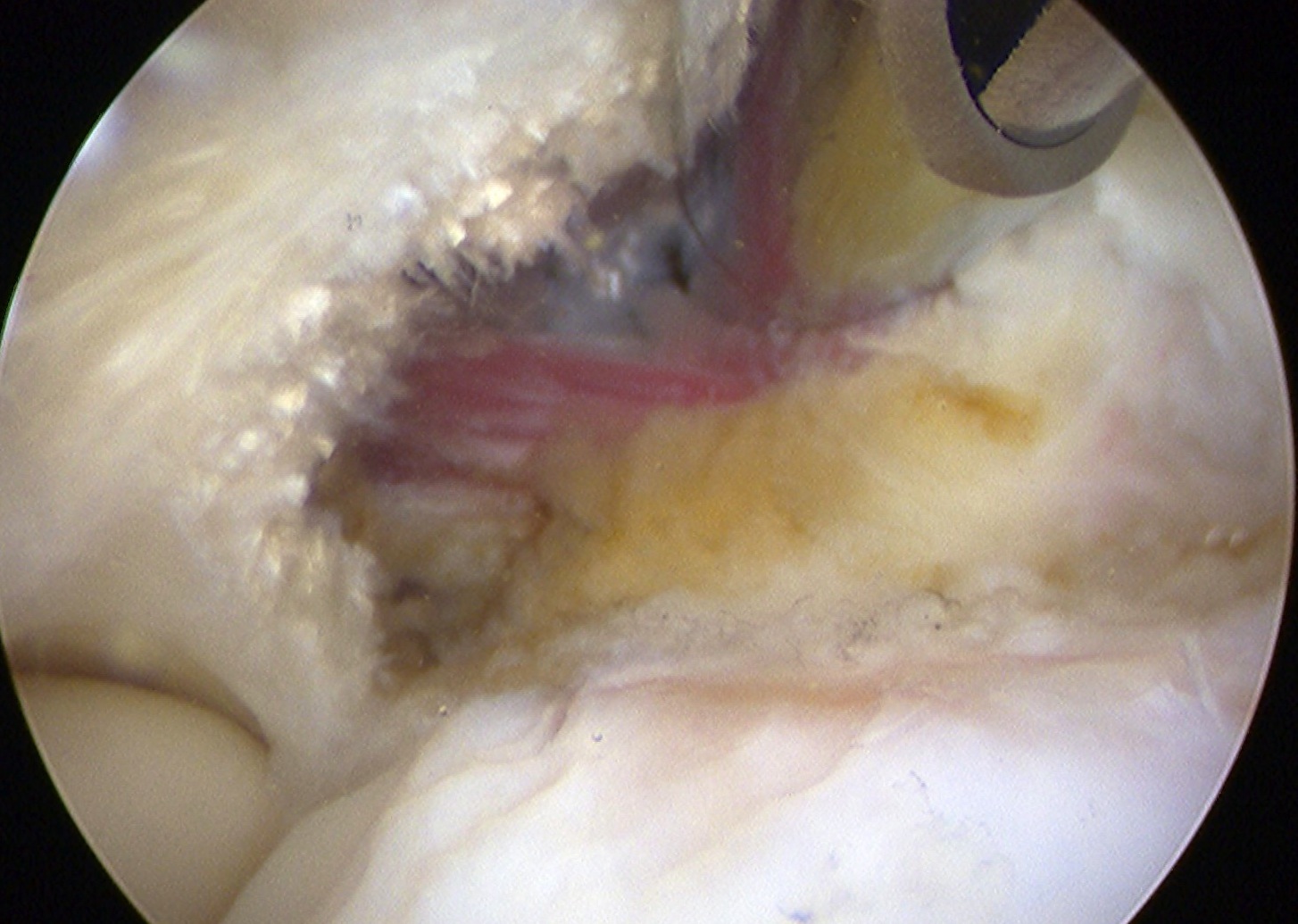
Arthroscopic Release

Complications
Instability
- inadvertant release LCL
Neuroma
- posterior cutaneous nerve forearm
- runs 1.5 cm anterior to lateral epicondyle on BR fascia
HO
- rare, but can be devastating
Results
Dunn et al Am J Sports Med 2008
- retrospective study of 92 elbows over 12 years
- open release
- 84% good to excellent results
Baker et al Am J Sports Med 2008
- 42 patients with arthroscopic resection followed up for 10 years average
- 87% patient satisfaction
Dunkow et al JBJS Br 2004
- RCT open v percutaneous tenotomy
- earlier return to work and faster recovery
Meknas et al Am J Sports Med 2008
- RCT of open release v microfrequency tenotomy
- no difference in pain relief
- better grip strength at 12 weeks