Epidemiology

6 /100 000
- second most common dislocation after shoulder
Mechanism
FOOSH
Goal
1. Obtain and maintain a concentric reduction
2. Achieve a painless and functional ROM
Associated Injuries
20% neuropraxia (ulna nerve / AIN)
Classification
Final position of Ulna Relative to Humerus
Posterior
Posterolateral
Degree
1. Complete
2. Subluxed / Perched (Drop sign)
- < 10 % patients
Simple / Complex
25-50% associated with fracture
Timing
Acute / Chronic / Recurrent
Bony Anatomy
Ulnohumeral Joint
Trochlea and ulna highly conformed
- trochlea covered by cartilage in arc 300o
- trochlea separated from the capitellum by groove in which rim of radial head articulates
- trochlea 6o valgus which creates carrying angle
Radiocapitellar Joint
60% of load at elbow
- concave radial head with capitellum
- posteromedial 2/3 articulates with sigmoid notch ulna
- anterolateral 1/3 has no cartilage / safe zone
Anterior part of radial head fractures normally
- part of spectrum in dislocation
- radial head important secondary stabiliser, especially when MCL deficient
Radial head and neck form an angle of 15o with the shaft
Distal Humerus
Tilted anteriorly 30o in lateral plane
- 5o internally in transverse plane
- 6o of valgus in front plane
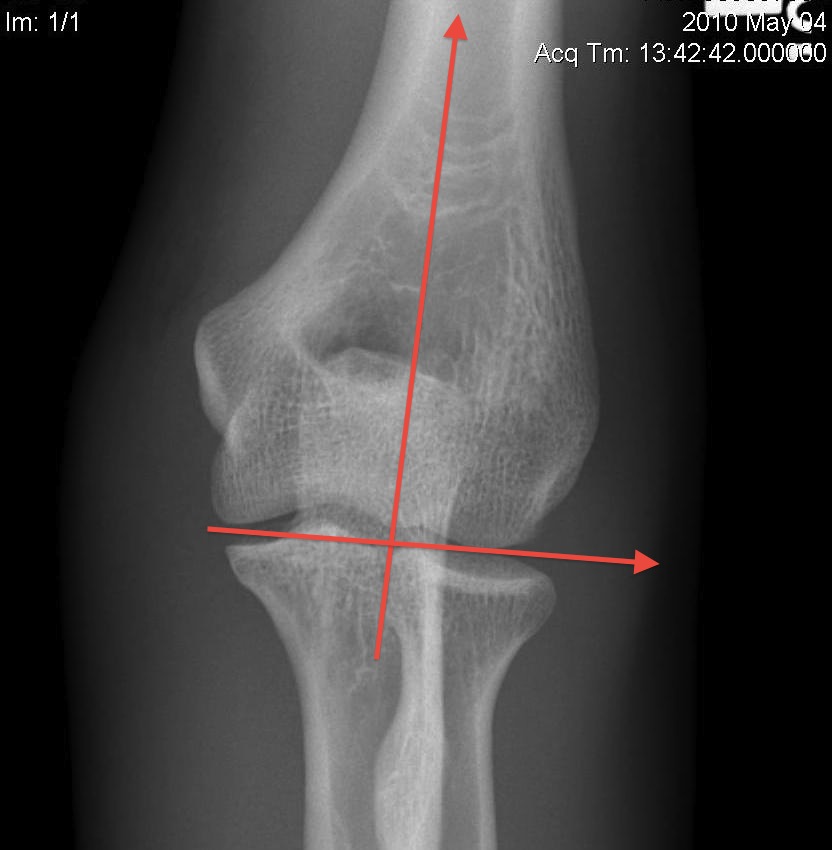

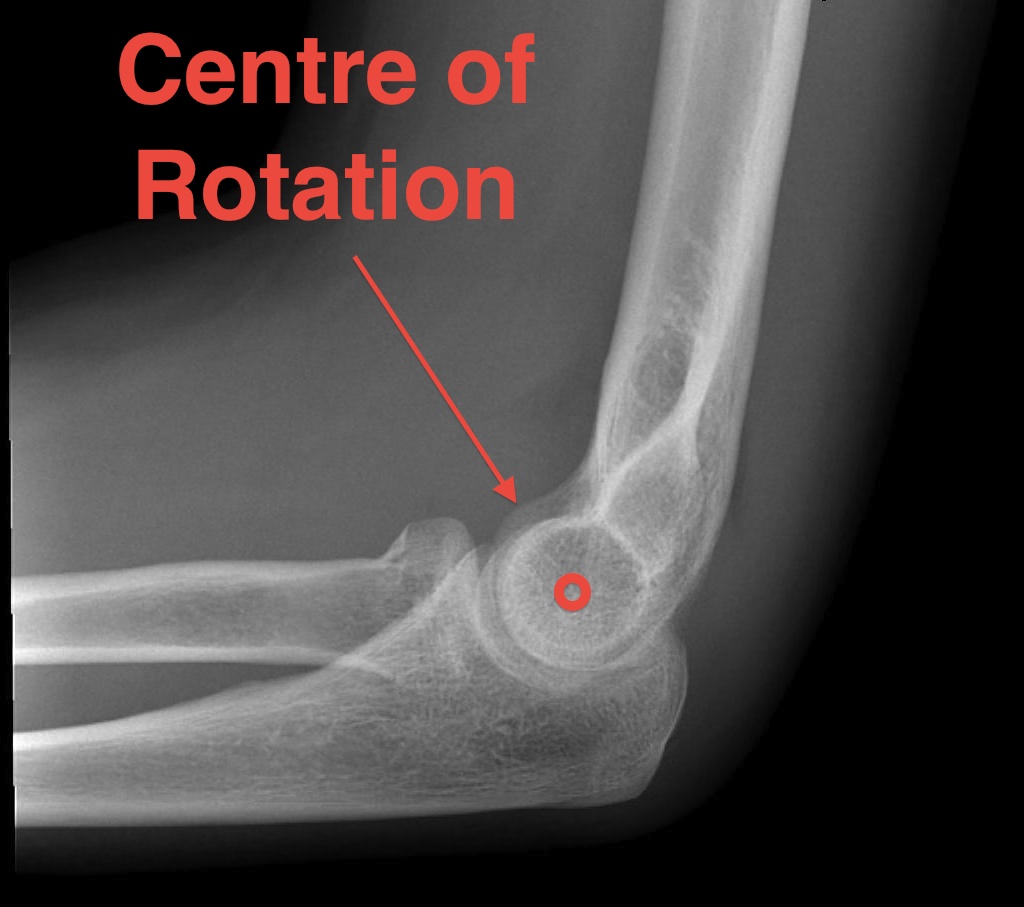
Centre of rotation
- trochlea
- centre of rotation offset anteriorly from humeral shaft
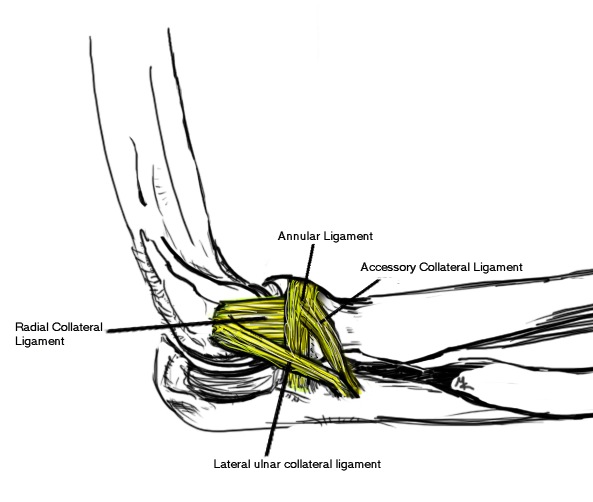
LCL
Action
- Varus Stability
LCL has 4 Components
1. Annular Ligament
- anterior edge supinator crest to posterior edge
2. Radial Collateral Ligament
- CEO to annular ligament
- fan-shaped
3. Lateral Ulna Collateral Ligament
Most important restraint to PL instability
- CEO to supinator crest
Must protect in Kocher approach
- in line with edge of anconeus, deep to it
- must protect in surgical approach between anconeus and ECU
4. Accessory Collateral Ligament
- from crest to diffusely over annular ligament
MCL

Action
- primary restraint to valgus stability
- especially in flexion
- this is the position in the throwing athlete
- in extension radial-capitellar joint important
3 parts
1. Anterior band
- CFO to sublime tubercle
- most important
2. Transverse band
- olecranon - sublime
- groove for ulna nerve
3. Posterior band
- CFO to olecranon
Constraints to Elbow Instability
Primary Static
1. Ulnohumeral articulation
- olecranon and coronoid
2. MCL
3. LCL
Secondary Static
1. Radio-capitellar joint
2. CFO / EFO
3. Capsule
Dynamic Stabilisers
Anconeus - PLR stability
Triceps / Brachialis / Biceps
Pathoanatomy / Horii circle
Begins on the lateral side, progresses to the medial side in three stages
- anterior band of MCL is the last torn
Stage 1
Damage to LCL
- Posterolateral Rotatory Subluxation
- this can reduce spontaneously
Stage 2
Damage to anterior and posterior capsule
- posterior capsule quite insignificant
- anterior important
Coronoid appears perched on trochlea
- incomplete PL dislocation
- concave medial edge of ulna on trochlea
- can be easily reduced or even by patient
Stage 3
Medial disruption
Stage 3A
Anterior band of MCL intact
- postero-lateral dislocation
- pivots about this anterior band
- often seen with radial head and coronoid fracture
Reduce with traction, varus and pronation
Maintain stability with hand pronated
- stability provided by anterior MCL
Stage 3B
Entire MCL disrupted
- varus / valgus / rotatory instability present after reduction
Need to be flexed > 30 - 40o to be stable
Stage 3C
Unstable at 90o
Entire distal humerus stripped / CFO / CEO
- reduction maintained only with flexion > 90o