

Indications
1. Persistent instability despite ORIF and LCL repair
2. Gross acute instability, not suitable for surgery
3. Delayed treatment > 4 weeks
Compass hinge / S&N
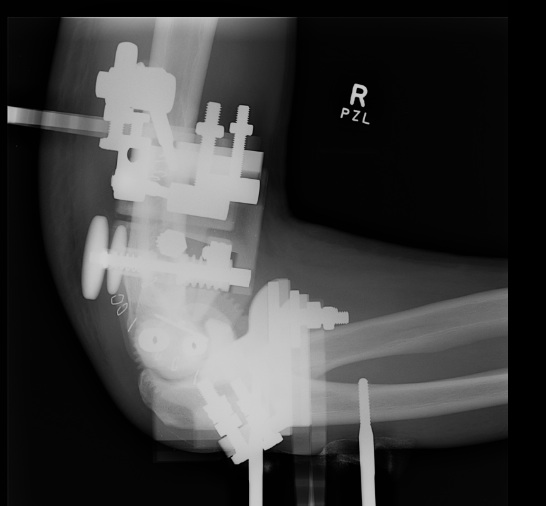
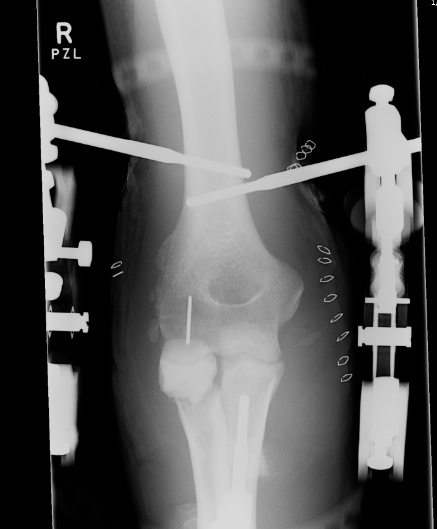


Set up
- two incomplete rings proximal and distal
- hinge in centre
- can be used actively or passively
- adjustment wheel is medial (to use with other hand)
- rings posterior, open anteriorly
- rings compatible with ilizarov equipment
- hinge can also be adjusted in the varus valgus plane
- do so that distal ring is perpendicular to plane of ulna

Key is distal humeral axis
- imagine axis is in spool at end of humerus
- open laterally to identify capitellum
- open medially to identify trochlea
- confirm centre of rotation on lateral
A. Insert medial and lateral 3.5 mm pins partially
- place external fixator over pins but this can be difficult
- adjust pins so hinge slides easily over them
- insert pins 2mm
B. Insert a single pin through axis of rotation
- slightly easier to apply the external hinge over the pin
- may not have to open the medial side as much
- only slight to identify and protect the ulna nerve
Medial Humeral half pin
- posterior to ulna nerve
- ensure proximal ring is perpendicular to humerus
- use two hole rancho cube with centering sleeve
- drop off undersurface off ring
- insert 5mm pin (drill, measure, insert HA pin by hand)
- need bicortical fixation
Lateral humeral pin
- anterior to radial nerve
- 2 hole post with single hole rancho
- allows angulation of pin from proximal to distal
- also angle posterior to anterior
Ulna pins
- 4mm pins into subcutaneous border
- must reduce elbow first and hold reduced whilst inserting pins
- ring must be perpendicular to ulna
- usually put elbow in 90 degrees of flexion
- proximal pin off proximal side of ring wth rancho cube
- bicortical usually into coronoid
- check is stable reduction
- insert second +/- third pin distally